
Inspiration
What do I want to be when I grow up?
John McGrory
I am a medical student nearing the end of my third year, and I still have no idea what residency I want to pursue after medical school. For those of you who are blissfully unaware of the intricacies of this exciting, yet daunting transition in medical education, I’m really getting low on time. I think it’s safe to say that I’ve graduated from the “cute and inquisitive” exploration stage and am rapidly approaching the “OK, this guy has some serious commitment issues” stage. I can’t quite put a finger on when this transition took place, but I think it was right around the time that my well-rehearsed, equivocal response to the oft-repeated specialty inquiry started to elicit concerned looks and hurried, probing questions instead of the “Oh, you have plenty of time” that I had gotten used to. I admire and envy the growing group of my colleagues that have firmly established their choice for this next step in their career. I imagine that this decisiveness extends to all facets of their lives: they’re probably able to select a movie within seconds of opening Netflix and have no trouble choosing a venue for group dinners. How nimble they must be when they are picking out their outfits in the morning and when they send texts to their crushes. Although each new convert to this group turns up the internal pressure on my decision-making, each one also serves to inspire. Clarity, however elusive, is apparently achievable.
So, how does one decide? “Find out what’s important to you, explore the different options, and choose what fits your needs and desires best.” “Find your people.” “Figure out which specialty’s ‘bread and-butter’ can keep you interested and engaged.” “Do what feels right.” “Ask a mentor for input; they know you best.”
All sage advice, and all heeded to the best of my ability and circumstances. Although
insight-provoking, this guidance has just felt a little too subjective to me. I’ve been described as a numbers guy, and all this talk about “feel” and “fit” came off as hopelessly abstract. So, in hopes of shedding some light on my future, I’m going to attempt to make this decision in a little more quantifiable terms. In fact, I’m going to throw some math at it. Now I’m not desperate enough (yet) to believe that all I’ve been missing thus far is a simple calculator. However, I think plainly laying out the different components that feed into this multidimensional decision will help to sort through my thought process and, hopefully, help illuminate the next step in my professional journey.
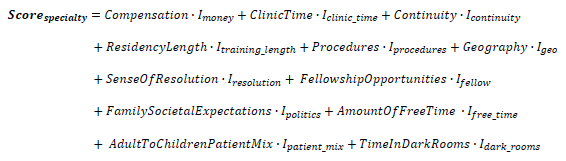
The way I see it, there are several objective-ish elements of each specialty, including, for example, post-training compensation range, amount of clinic time, degree of continuity in one’s patient population, etc. On the student side, there are associated “importance” values that indicate how significant each factor is for that student in the decision. Examples could include importance values like Imoney, which if high, demonstrates a student highly valuing income, or Iclinic_time, which if negative, would mean that the student would rather write reflective essays all day than spend their working hours hanging out in a clinic. For a particular specialty, if we multiply each factor’s score by the student’s perceived value of that factor and sum all of them, we can obtain a score for that specialty. Rinse and repeat for all the different specialties , and the highest score wins. Simple, right? Let’s see what a general equation might look like:
To give an example for a particular specialty, one could describe family medicine, again in objective-ish terms, as a specialty with high clinic time, high continuity, and low relative residency length. Neurosurgery could be described as having low to moderate clinic time, high residency training length, high proportion of procedures, and a low amount of free time. There are, of course, nuances in how different programs within one specialty approach training and work-life balance, but for the sake of keeping this thing readable, let’s assume all programs within a particular residency are roughly equal.
Some of these factors may not be intuitive, so let’s break them down a little further. What is “sense of resolution”? I envision this as a metric that captures that feeling one gets when flipping over a flash card or figuring out the solution to a riddle. Physicians of all walks spend a great deal of their time making guesses with limited information; the higher a specialty’s sense-of resolution score, the more likely you are to actually get a “thumbs-up” or “thumbs-down” at the end of your investigation. I think an exemplar for the lower end of this spectrum would be emergency medicine, whereas one could argue that specialties like pathology or surgery might be nearer the high end.
“Family and societal expectations” is something I threw in there for people with a family lineage full of urologists that might perceive their descendant’s choice to pursue pediatrics as a denouncement of their life choices. I think it could also encompass society’s assumptions about what type of people belong in different specialties, for example, the intersection of gender and an OB/Gyn residency or the politics surrounding midlevel practitioners encroaching on that specialty’s scope of practice. How about geography? Maybe Wyoming is your jam and you just can’t picture yourself anywhere else. Well, then Igeo is going to be pretty high, and you’ll be vying for one of those 14 family medicine spots available every year in the Cowboy State.
I think you get it. Let’s work through an example and see how this equation performs. For the importance values, I’ll use a fictitious example for the undecided student. Let’s call him “John”. Before we begin, a quick request for the reader: please forgive the massive generalizations about various specialties in the next couple of paragraphs. They are the result of equal parts convenience, rationalization, and ignorance.
Now John’s most important values are probably |clinic_time, |resolution, |procedures, |free_time, and |dark_rooms. He digs using his hands; he values his free time away from the hospital/clinic; uncertainty is lower on the list, but he’d rather get an answer than be left hanging; dark rooms kind of freak him out; and the clinic isn’t exactly his idea of a good time. Now, let’s peruse our specialty chart. It looks like ClinicTime in family medicine is off the charts, so let’s go ahead and veto that. Neurology has a higher clinic time and scores on the low end of SenseOfResolution, so we’ll scrap that too. Checking out the AmountOfFreeTime column makes him pretty comfortable with dropping all of the surgical specialties. Apart from the little bump from ECTs, I’m not seeing a lot under psychiatry that would scratch that |procedures, itch, so we can throw that out, as well. Same with pathology, allergy/immunology, and medical genetics. And even though radiology is pretty neat, John’s negative |dark_roomsvalue is going to preclude it as a career choice.
So, where does that leave us? Anesthesiology, emergency medicine, internal medicine, OB/Gyn, pediatrics, and PM&R. So, we ask John about his more minor importance values. He likes working with kids, but |patient_mix is somewhat important, so I think we can cross out pediatrics. He doesn’t have much experience with PM&R, so to the back burner it goes. Other than AmountOfFreeTime, OB/Gyn actually scores pretty well – we’ll defer judgement for now. |resolution is making him think hard about canning emergency medicine, but its score is otherwise fairly high. Anesthesiologists usually seem happy with their high Compensation and Procedure values, but it has to get kind of lonely behind that curtain; also, as the specialty that’s arguably most affected by midlevel creep, |politics feels like it’s becoming a factor. What about the ultimate fallback, internal medicine? It’s tough to grade this one since there are so many paths available after residency. John’s a non-traditional student though, so that increases the importance of |training_length. It’s becoming clear that we probably won’t land on a single answer for “John”, but I think the process forced him to delineate what’s important to him in his personal and professional life. After objective analysis, It’s easier to start applying the “feel” and “fit” concepts with a manageable list of 3-4 specialties instead of 30-40. With this potent knowledge obtained via the neurotic hyper-analyzation known to most medical students, he’s sure to figure it all out very soon. Right?
For those of you who are reading this and find yourself alongside me in Camp Indecision, I hope this breakdown has helped you to organize your thoughts. If not, then hopefully you at least found my ramblings entertaining. I will conclude with an attending’s piece of advice that has stuck with me throughout this endeavor: “There is no perfect answer.” I’m beginning to accept the fact that this decision will not be made as a result of an epiphany, nor from a “precise” distillation of my values with respect to inaccurate but quantified specialty attributes, but rather as a product of much introspection, internal and external deliberation, and a little bit of luck.
References
https://freida.ama-assn.org/