
6 Abdomen 1: Equine and Porcine
Revised Spring 2024 by T. Clark
Additional Resources for this Chapter:
- Related Supplemental Large Animal Surgery links:LAS Colic pathophysiology; LAS Gastric lesions; LAS Impactions – Cecal, Colon and Small Colon; LAS Impactions – stomach and small intestine
- Veterinary Gross Anatomy Ungulate Dissection (Abdomen Labs 11-14)
- Helpful Dissection Videos:
- Dried Equine Stomach (3:06)
- Dried Equine Large Intestine (2:42)
- Dried Porcine Stomach (2:34)
- Dried Porcine Cecum (0:39)
- Embalmed Equine Abdominal Viscera (21:39)
- Fresh Equine Abdominal Viscera (12:44)
Objective
A6.1 Identify and describe the structures and organs of the abdomen in equine; describe the normal topography of the abdomen and localize the related internal and external structures and organs.
Abdominal Wall Muscles and Structures
- The abdominal wall is mostly muscular and tendinous and includes the external abdominal oblique mm., the outermost muscular layer. The tunica flava abdominis is a pale yellow elastic sheet of deep fascia covering this muscle. It assists the abdominal muscles in supporting the weight of the abdominal viscera
- The rectus abdominis mm. are bilateral muscles running along the ventral midline of the abdomen and insert on the pubis via the prepubic tendon. The prepubic tendon is the connective tissue insertion of the abdominal muscles onto the public bones.
- The middle muscular layer of the abdominal wall is the internal abdominal oblique mm., while the deepest is the transversus abdominis mm.
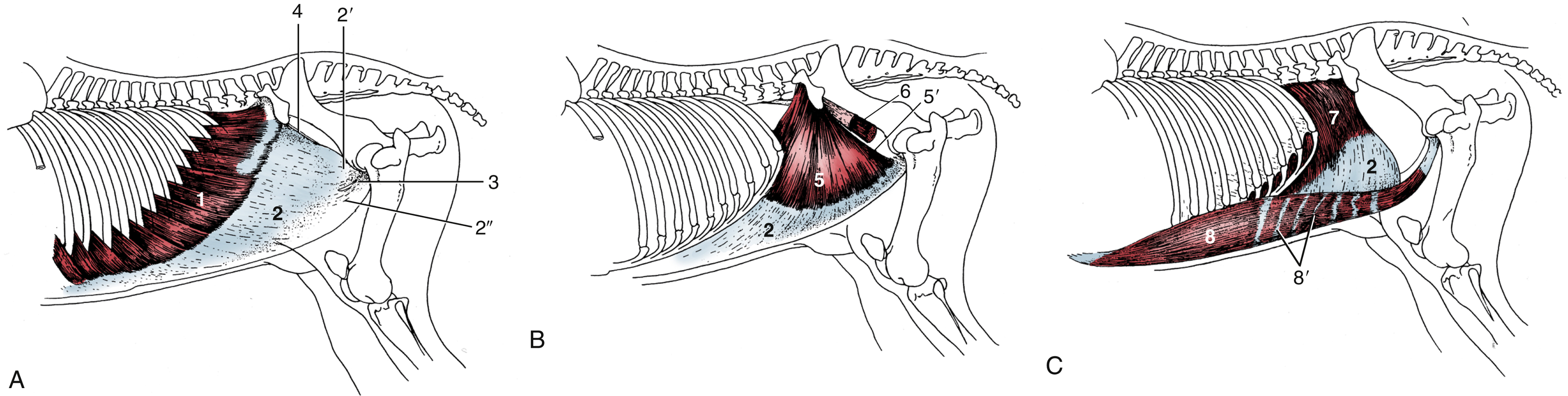
FIG. 21.1 The abdominal muscles and their skeletal attachments in equine. 1, External abdominal oblique, muscular part; 2, aponeurotic parts of 1, 5, and 7; 2′ and 2″, pelvic and abdominal tendons of aponeurotic part, respectively; 3, superficial inguinal ring; 4, attachment of pelvic tendon of external oblique aponeurosis on iliopsoas and sartorius (“inguinal ligament”); 5, internal abdominal oblique, muscular part; 5′, free caudal border forming the cranial margin of the deep inguinal ring; 6, iliopsoas, partly enclosed by iliac fascia; 7, transversus abdominis, muscular part; 8, rectus abdominis; 8′, tendinous inscriptions. TVA
- The subiliac lymph node (bov) / subiliac lymphocenter (eq) is found at the cranial edge of the thigh muscles, about midway between the tuber coxae and the fold of the flank. (Fig. 31.10)
- The paralumbar fossa (ID in bov, but also present in eq) is the most common surgical site for entry into the ruminant abdomen. It is a triangular depression bounded by lumbar transverse processes and the epaxial muscle dorsal to the processes, the last rib, and an oblique muscular thickening of the internal abdominal oblique m. extending from the tuber coxae to the costal arch. (see image below)
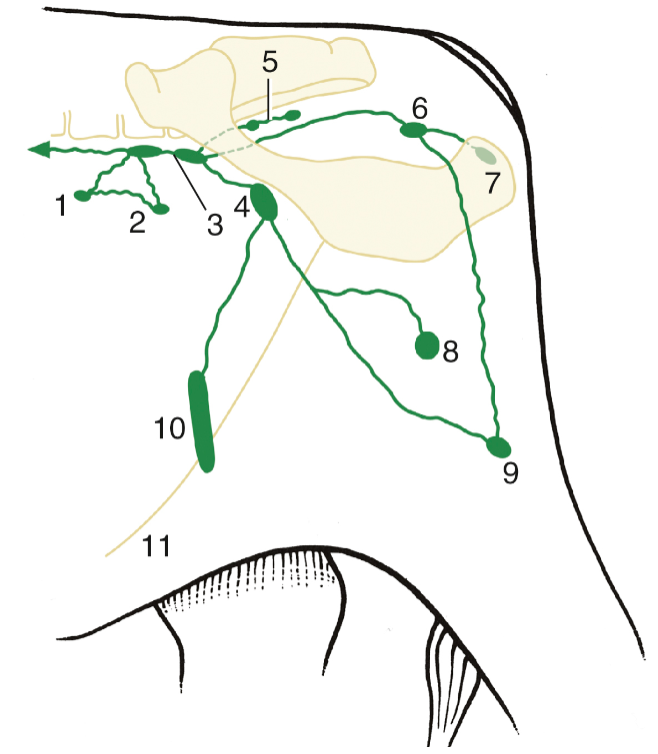
FIG. 31.10 The lymph nodes of the bovine pelvis and hindlimb. 1, Lateral iliac lymph node; 2, coxal lymph node; 3, medial iliac and sacral lymph nodes; 4, deep inguinal lymph node; 5, gluteal lymph node; 6, ischial lymph node; 7, tuberal lymph node; 8, superficial inguinal (mammary) lymph node; 9, popliteal lymph node; 10, subiliac lymph node; 11, linea alba. TVA

Figure above – stethoscope placed in the left paralumbar fossa of a bovine.
Abdominal Membranes and Other Structures
- The abdominal cavity is formed by the muscles of the abdominal wall, the ribs, and the diaphragm; it is lined by peritoneum, which encloses the peritoneal cavity.
- The parietal peritoneum is the serous membrane lining the body wall, while the visceral peritoneum is directly on the surfaces of the abdominal organs.
- Connecting peritoneum connects the parietal and visceral layers, or the visceral layers of adjacent organs and can form peritoneal folds called ‘mesenteries’, ‘omenta’, or ‘ligaments.’
- The greater omentum and lesser omentum are connective tissues associated with the greater and lesser curvatures of the stomach.
- The mesoduodenum, mesojejunum, mesoileum, and mesocolon are mesenteries wrapping the duodenum, jejunum, ileum, and colon, respectively. The root of the mesentery is at the center of these mesenteries (and has the cranial mesenteric a. running within) and is a point of firm attachment to the dorsal body wall, however the small intestines are still relatively mobile.
- Typically in equine, there are several mesenteric lymph nodes near the root of the mesentery.
Figure (above) showing examples of mesenteries (e.g., mesocolon); the “root of the mesentery” is at the center of each figure of the GI tract.
-
- The nephrosplenic ligament connects the left kidney and spleen, the ileocecal ligament/fold connects the ileum and cecum, and the cecocolic ligament/fold connects the cecum and colon.
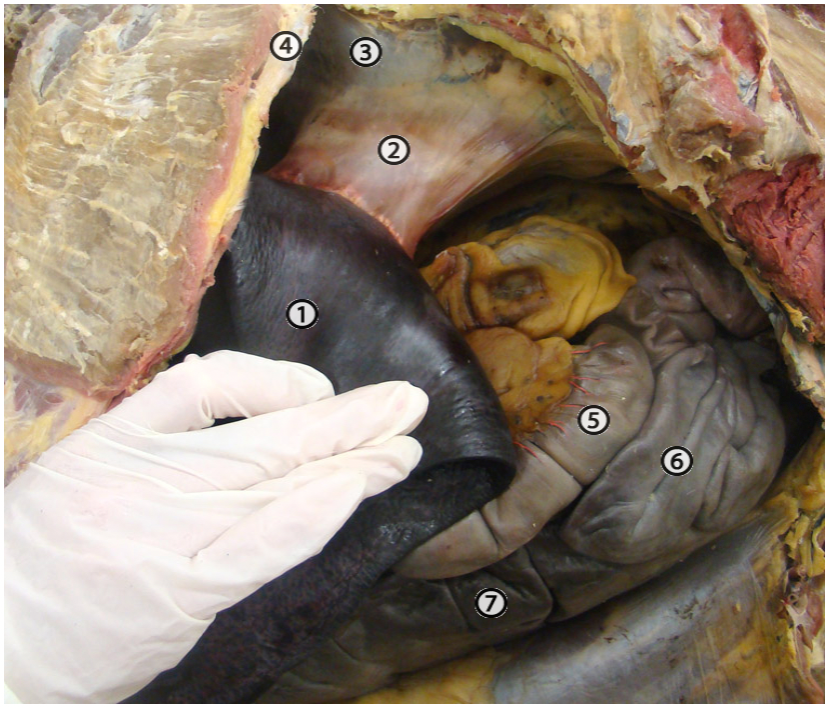
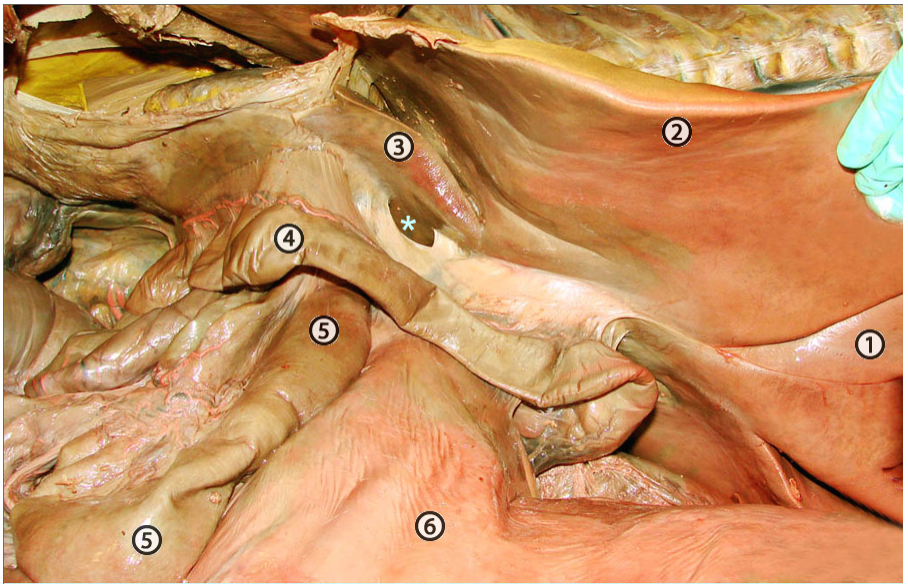
View of left equine abdomen, manual reflection of the base of the spleen (1) to expose the nephrosplenic ligament (2) and the left kidney (3). 4, last rib; 5, small colon; 6, small intestine; 7, left ventral colon. http://vanat.cvm.umn.edu/ungDissect/Lab13/Img13-6.html
- Liver
- EQUINE: the horse does not have a gall bladder, but does have a bile duct. The liver lobes are left lateral, left medial, quadrate, right, and caudate. The round ligament helps to identify the separation between the quadrate and left medial lobes. The horse liver has less distinct lobations than the other species we have seen.
- Other species that do not have gall bladders: deer, rats, llamas, alpacas, vicunas, guanacos; several species of birds.
- PORCINE: the pig has a prominent gall bladder and has five to six liver lobes: right lateral and medial, quadrate, left medial and lateral, and caudate (caudate process).
- EQUINE: the horse does not have a gall bladder, but does have a bile duct. The liver lobes are left lateral, left medial, quadrate, right, and caudate. The round ligament helps to identify the separation between the quadrate and left medial lobes. The horse liver has less distinct lobations than the other species we have seen.
- The portal v. delivers nutrient and metabolite dense blood to the liver for filtering. The hepatic vv. exit the liver and empty into the caudal vena cava.
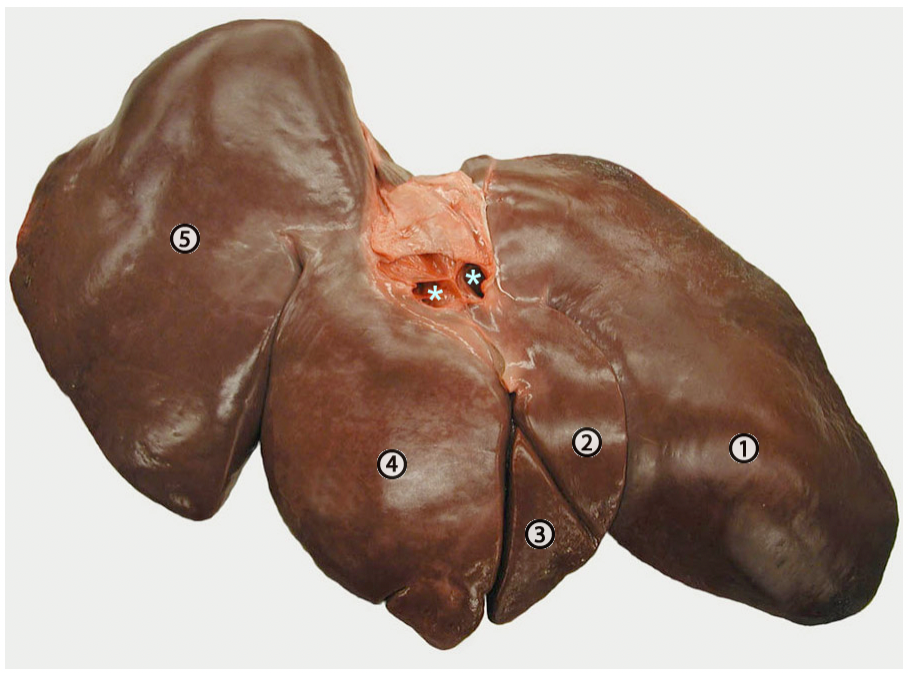
Diaphragmatic surface of the equine liver. 1, left lateral lobe; 2 & 3, left medial lobe; 4, quadrate lobe; 5, right lobe; asterisks, hepatic veins near their entrance into the caudal vena cava (not shown). http://vanat.cvm.umn.edu/ungDissect/Lab13/Img13-17.html
- Within the wall of the duodenum, there is a major duodenal papilla, which allows the bile duct and main pancreatic duct to enter into the duodenum.
- On the opposite wall of the duodenum from the major papillae, there may also be a minor duodenal papilla (the point where an accessory pancreatic duct may enter into the duodenum).
- The pancreas is dorsal to the lesser curvature of the stomach and runs along the proximal portion of the duodenum. Much of it is nestled in the mesoduodenum and is situated relatively dorsally making it hard to find if the GI tract is still attached to the dorsal abdominal wall.
- The left and right kidneys are tucked in fat and hidden along the dorsal body wall (i.e., retroperitoneal). The left kidney is near the base of the spleen, while the right kidney is near the base of the cecum.
- Inside the kidney, the outer layer is the cortex and the inner portion is the medulla.
- The renal pelvis is the expanded part of the ureter within the kidney. The ureters extend from each kidney to the caudal portion of the urinary bladder.
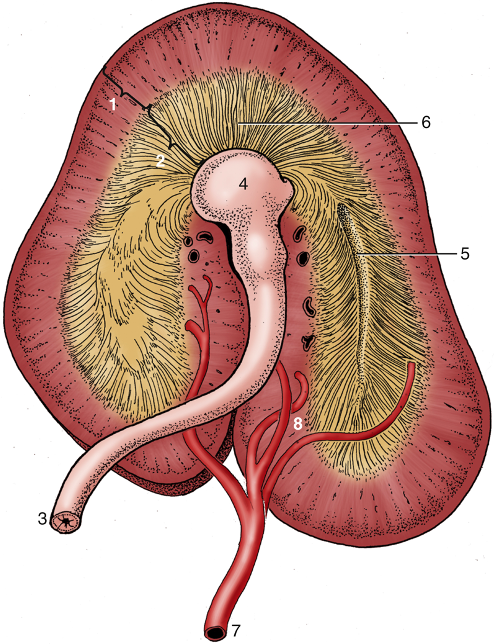
FIG. 21.23 Dorsal section through an equine kidney (semi-schematic). 1, Renal cortex; 2, renal medulla; 3, ureter; 4, pelvis; 5, terminal recess; 6, papillary ducts; 7, renal artery; 8, interlobar arteries. TVA
- From the abdomen, you may be able to view structures of the pelvis. The pelvic brim is the cranial edge of the pelvis/pubic region at the pelvic inlet.
- In females, the uterus (uterine horns, uterine body) and ovaries may be found in the caudal and lateral abdominal area.
- In males, the paired ductus deferens may exit near the vaginal ring and deep inguinal ring in the caudal and ventral abdominal wall.
- The urinary bladder is the ventral-most organ in both males and females in the caudal abdomen near the pelvic inlet.
Equine Abdominal Topography – note a large amount of abdominal organs are covered by the ribs, indicating these organs project into the thoracic space.
- Left side structures/organs in EQUINE:
- The spleen has a base (more dorsal) and apex (more ventral), and hugs part of the greater curvature of the stomach.
- The left kidney is near the dorsal body wall and is encased in fat. The nephrosplenic ligament connects the left kidney and spleen. The kidney can be visualized on ultrasound.
- The fundus portion of the stomach is normally more towards the left side.
- The left dorsal colon (LDC), left ventral colon (LVC), and pelvic flexure of the ascending colon are found on the left.
- Most of the jejunum and descending/small colon are found more towards the left.
- The ileum enters the left side of the cecum at midline.
- A small portion of the left lobe of the liver is on the left.
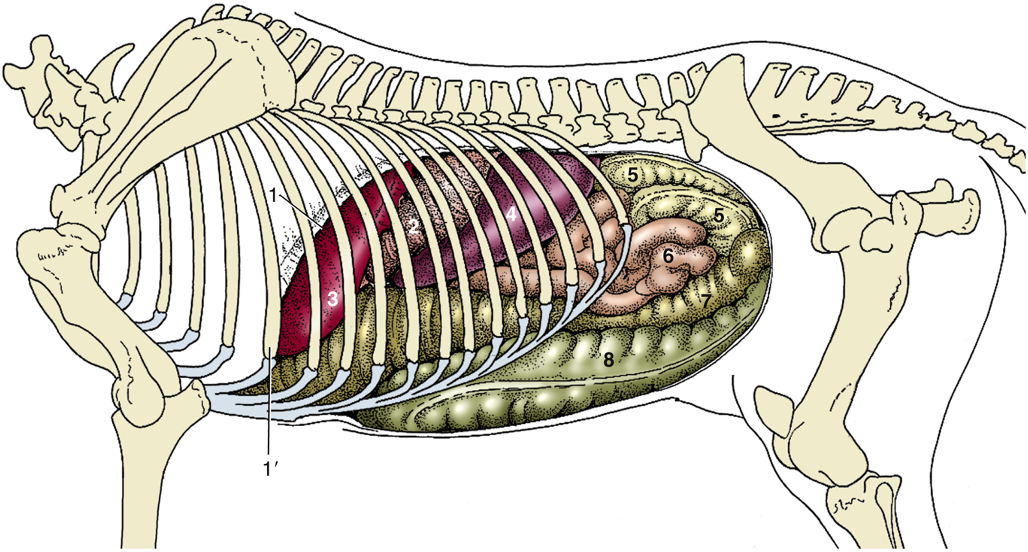
FIG. 21.6 Visceral projections on the left equine abdominal wall (including the diaphragm). 1, Cut edge of diaphragm; 1′, rib 6; 2, stomach (fundus); 3, liver (left lobe); 4, spleen; 5, descending/small colon (banded); 6, jejunum (smooth); 7, left dorsal colon; 8, left ventral colon. TVA
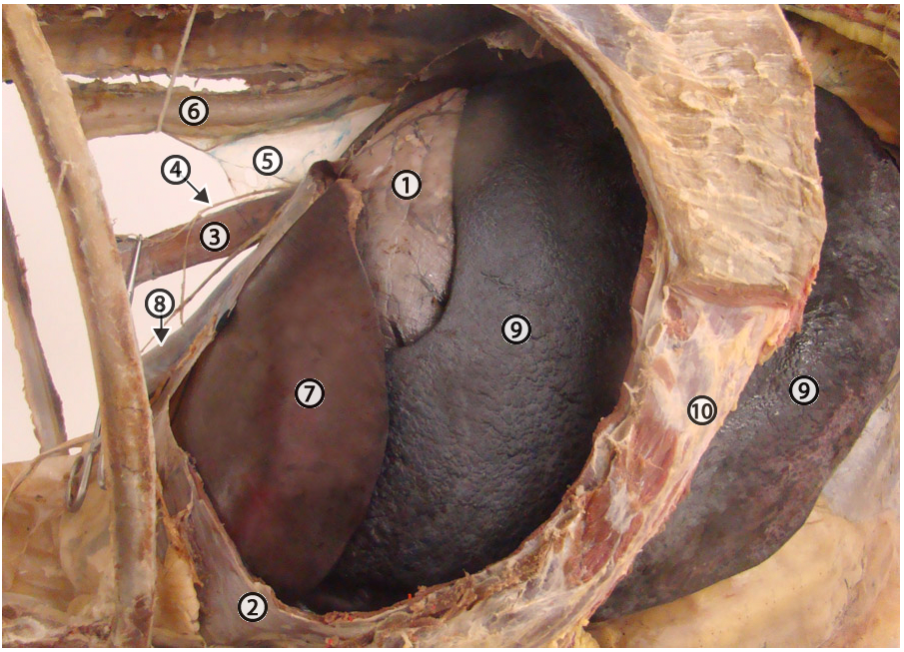
Left view of equine abdomen – exposure of the stomach (1) through a large window cut in the diaphragm (2). The spleen (9) is enlarged due to use of barbiturate anesthesia for euthanasia. 3, esophagus; 4, dorsal vagal nerve trunk; 5, mediastinal pleura; 6, aorta; 7, left lateral lobe of the liver; 8, caudal vena cava; 10, costal arch. http://vanat.cvm.umn.edu/ungDissect/Lab13/Img13-2.html
- Right side structures/organs in EQUINE:
- The base (dorsal portion or top of the “comma”) and some of the body of the cecum can be found on the right.
- Most of the liver (right and quadrate lobes) takes up the right side of the abdomen and some of the ventral abdomen. The liver can be visualized on ultrasound.
- The pyloric portion of the stomach is normally on the right.
- The descending duodenum, which runs dorsally, and the epiploic foramen (deep to the liver, opens into the omental bursa) are found on the right.
- The right dorsal colon (RDC) and right ventral colon (RVC) of the ascending colon are on the right.
- The cecocolic ligament/fold is found between the cecum and colon.

FIG. 21.7 Visceral projections on the right equine abdominal wall (including the diaphragm). 1, Cut edge of diaphragm; 1′, rib 6; 2, liver (right, quadrate lobes); 3, right kidney; 4, descending duodenum; 5, body of cecum; 6, right ventral colon; 7, right dorsal colon. TVA
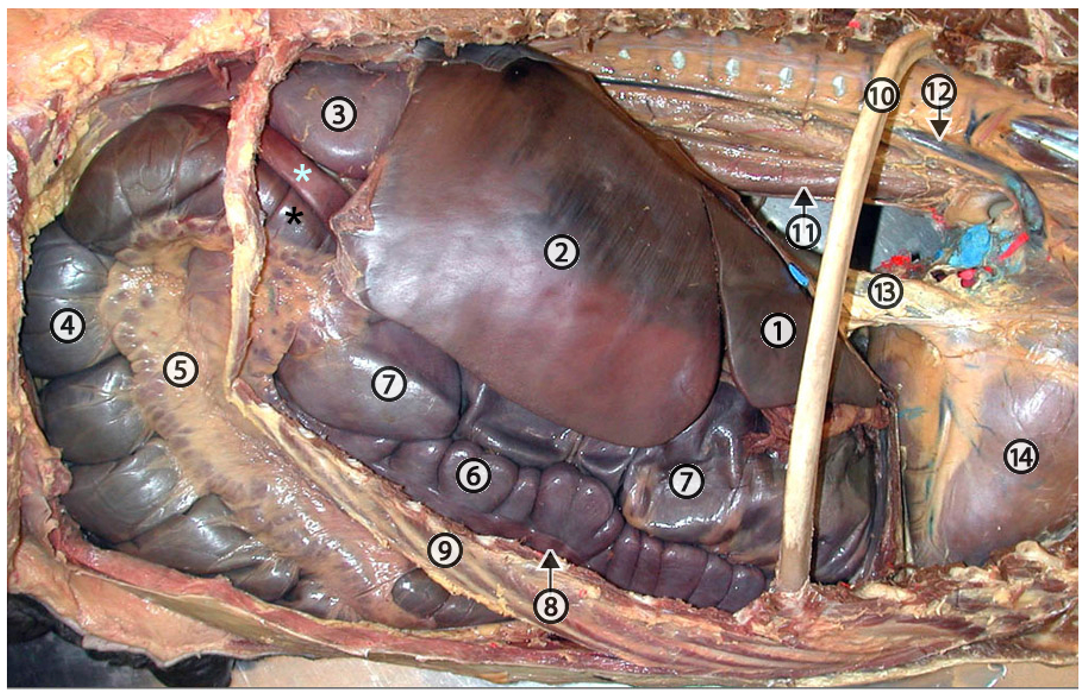
Exposure of abdominal viscera on the right side (equine). 1, quadrate lobe of liver; 2, right lobe of liver; 3, right kidney; blue asterisk, descending duodenum; black asterisk, base of cecum; 4, body of cecum; 5, cecocolic fold with abundant lymph nodes; 6, right ventral colon; 7, right dorsal colon; 8, intestinal band; 9, costal arch; 10, rib 7; 11, esophagus; 12, azygous vein; 13, caudal vena cava; 14, right ventricle. http://vanat.cvm.umn.edu/ungDissect/Lab13/Img13-7.html
Table 5-1 (from LA Dissection eBook) Major structures to be palpated/seen on each side of the equine abdomen.
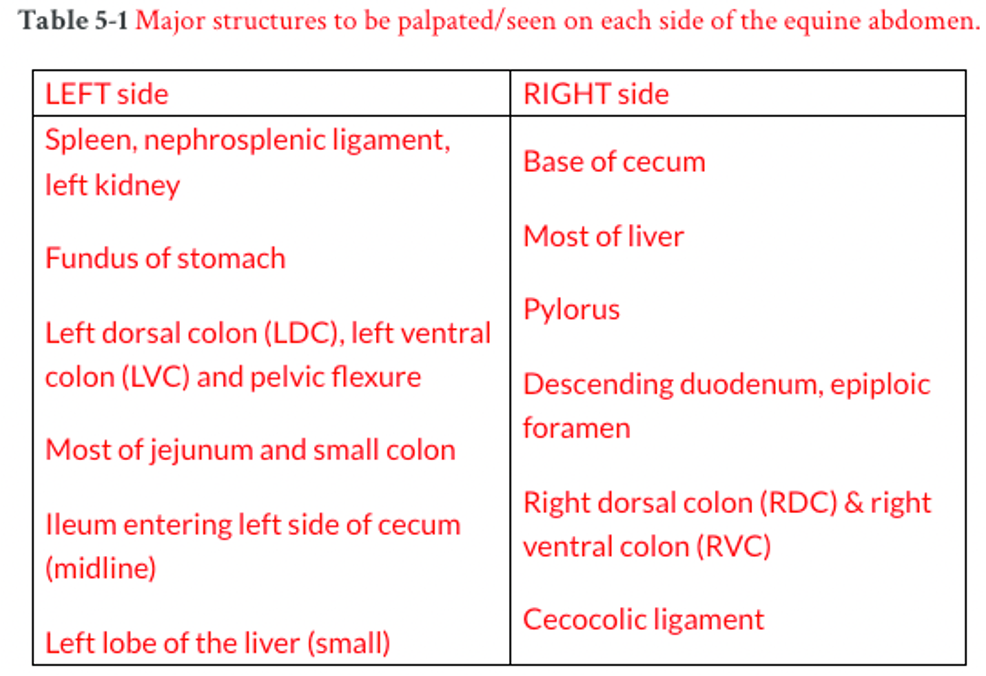
Note: upon rectal palpation of equine, you should be able to palpate the nephrosplenic space and ligament on the left, the cecum on the right, and differentiate the small colon from the ascending colon and small intestines.
Objective
A6.2 Summarize the regions of the gastrointestinal tract that are supplied by the celiac and cranial mesenteric arteries in the equine.
- The arterial pattern in large animals is similar to carnivores, where the main branches of the abdominal aorta include the: celiac, cranial mesenteric, and caudal mesenteric arteries.
- The celiac a. is unpaired and provides blood to viscera in the cranial abdominal cavity (i.e., foregut) via the:
- Splenic a. to the spleen and greater curvature of stomach.
- Hepatic a. to the liver, lesser and greater curvatures of stomach, and part of the pancreas and duodenum.
- Left gastric a. to the lesser curvature of the stomach and part of the pancreas.
- The cranial mesenteric a. is unpaired (runs within the root of the mesentery) and provides blood to viscera in the middle abdominal cavity (i.e., midgut) via the:
- Jejunal aa. to the intestinal mass (found in much of the root of the mesentery and mesojejunum).
- Right colic a. to the dorsal colon (and running along the dorsal colon). It meets the colic a. branch from the ileocolic a. at the pelvic flexure.
- Colic a. branch (of the ileocolic a.) to the ventral colon (and running along the ventral colon). The right colic a. and colic a. form an important arterial loop of the ascending colon.
- Arteries arising from the cranial mesenteric a. also supply the duodenum, pancreas, ileum, cecum, transverse colon, and initial part of the descending colon.
- Caudal mesenteric a. is unpaired and provides blood to viscera in the caudal abdominal cavity (i.e., hindgut) via the:
- Left colic a. to the descending colon.
- Cranial rectal a. to the initial rectum.
- Clinical Note: Strongylosis (caused by strongyles nematodes) is a relevant internal parasitic disease in EQUINE. These parasites can migrate to the cranial mesenteric a., cause a thrombus to form, and lead to reduced blood flow to the GI tract. Follow this link for more information about large and small strongyles. (Supplemental Clinical LAS Colic pathophysiology)
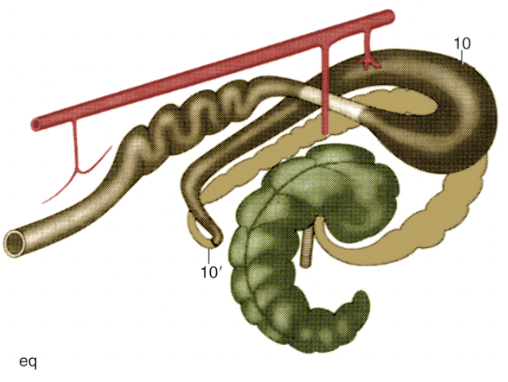
FIG. 3.45 Schematic drawing of the large intestine of the horse (eq). Cranial is to the upper right, flow (each segment is a different color): ileum; cecum; ascending colon; transverse colon; descending colon; rectum and anus; The aorta is along the top with the celiac artery and cranial and caudal mesenteric arteries; 10 and 10′, dorsal diaphragmatic and pelvic flexures of ascending colon. TVA
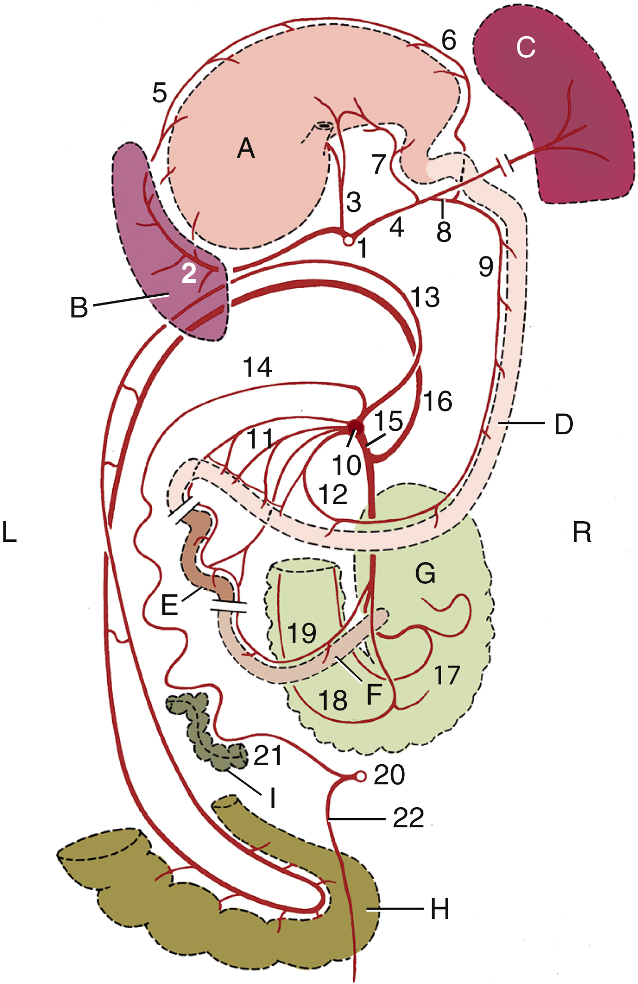
FIG. 21.20 The major arteries of the gastrointestinal tract (schematic), dorsal view. The structures have been stretched craniocaudally for clarity. (A) Stomach; (B) spleen; (C) liver; (D) duodenum; (E) jejunum; (F) ileum; (G) cecum; (H) pelvic flexure; (I) descending colon. 1, Celiac artery (a.); 2, splenic a.; 3, left gastric a.; 4, hepatic a.; 5, left gastroepiploic a.; 6, right gastroepiploic a.; 7, right gastric a.; 8,gastroduodenal a.; 9, cranial pancreaticoduodenal a.; 10, cranial mesenteric a.; 11, jejunal arteries; 12, caudal pancreaticoduodenal a.; 13, right colic a.; 14, middle colic a; 15, ileocolic a.; 16, colic branch of ileocolic a.; 17, lateral cecal a.; 18, medial cecal a.; 19, mesenteric ileal a.; 20, caudal mesenteric a.; 21, left colic a.; 22, cranial rectal a. TVA
Objective
A6.3 Identify and describe the anatomical features of the equine and porcine stomach; summarize notable species differences.
Equine Stomach (Figure 10B-1); There are dried, fresh, and preserved equine stomach specimens available in the gross anatomy lab.
- The esophagus enters the stomach near the cardia(c) region at an acute angle.
- There is a thick and strong sphincter in the wall of the cardia (aka cardiac sphincter, or lower esophageal sphincter).
- These two features (sphincter and acute angle) contribute to preventing HORSES from being able to vomit. This is why back up of ingesta into the stomach can be harmful for horses, and why a nasogastric tube is used to detect buildup of pressure.
- The fundus/fundic region is the rounded and bulging region adjacent to the cardia, which can become distended when food fills the stomach. The fundic region typically lies to the left of midline.
- The body of the stomach is the middle third, or central portion.
- The pyloric region/pylorus is the distal third, which has an antrum and canal that narrows. The canal ends with an orifice surrounded by the pyloric sphincter. The pylorus is typically right of midline.
- The curves of the stomach include the greater and lesser curvatures, which have greater and lesser omenta, respectively. Note the closeness of the cardia to the pylorus and hence the much-reduced lesser curvature of the stomach in EQUINE.
- The EQUINE stomach is divided into non-glandular and glandular regions.
- The non-glandular region is lined with stratified squamous epithelium and can appear white. This is mostly near the cardiac and fundic regions, and proximal portions of the body.
- The glandular region is lined with simple columnar epithelium and appears shiny. This is mostly found in the distal body and pyloric regions. These regions may have divots in the wall left from botfly larvae. (more about stomach bots in horses)
-
- The margo plicatus is the junction between the non-glandular and glandular regions of the stomach.
- Distal to the pylorus is the proximal part of the duodenum which has the major duodenal papilla (and minor duodenal papilla). The descending duodenum continues along the dorsal right side of the body (attached via the mesoduodenum), makes a turn near the right kidney via the caudal duodenal flexure/caudal loop before transitioning into the ascending duodenum (the jejunum is the next section of small intestine).
- Endoscopy can be performed on the equine esophagus and stomach to explore and visualize these regions for lesions and ulcerations. (Supplemental Clinical LAS Gastric lesions)
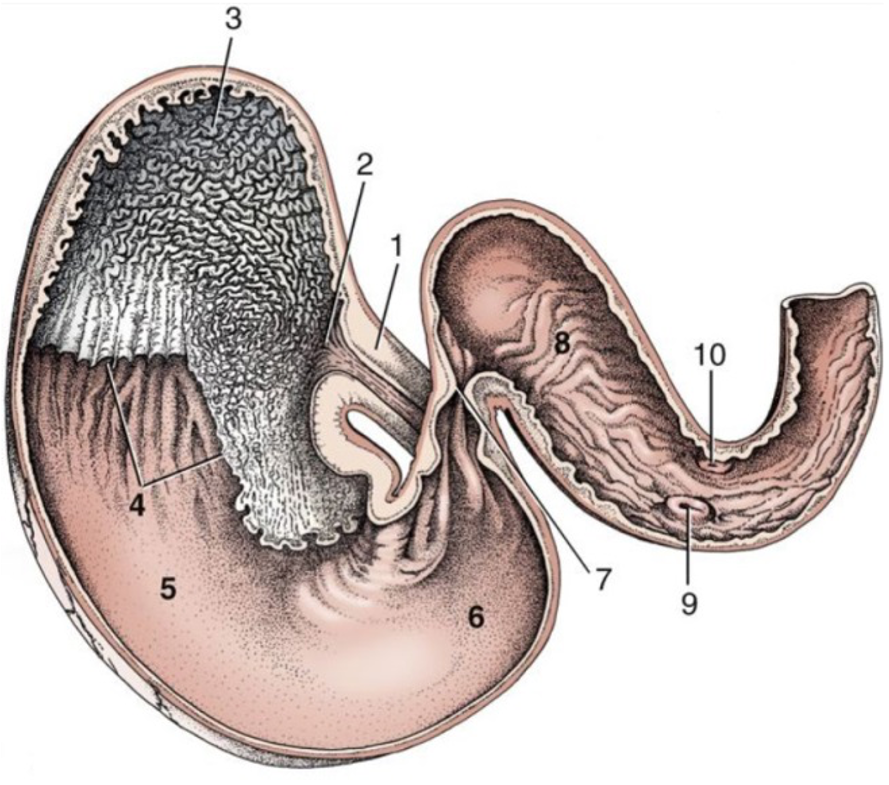
Figure 10B-1 (Above) Equine, ventral caudal view of the interior of the stomach and proximal part of the duodenum. 1, esophagus; non-glandular stomach regions: 2, cardiac opening/region and 3, fundus/fundic region; 4, margo plicatus; glandular stomach regions: 5, body and 6, pyloric region; 7, pylorus; 8, cranial part of duodenum (located on the right side of abdomen); 9, major duodenal papilla; 10, minor duodenal papilla. (Modified from TVA Fig. 21-9)
Porcine Stomach (some images from Ungulate Dissection Website)
- The PIG stomach is a simple stomach but has two distinctive structures: the gastric diverticulum and the torus pyloricus. (see images below)
- The gastric diverticulum is a noticeable bulge that protrudes from the fundus of the stomach. This is a blind pouch of the stomach that is distinctive in the PIG.
- The torus pyloricus is the prominence that narrows the lumen of the pyloric canal. This structure is a smooth muscle in the wall of the pyloric canal proximal to the pyloric sphincter. The added ridge helps control food (i.e., valve to seal or limit outflow from the stomach) as it enters the duodenum along with the pyloric sphincter. The torus pyloricus is found in RUMINANTS and PIGS.
- In the pig, the non-glandular region is much smaller than the HORSE and is only near the cardia (where the esophagus enters), while the glandular region covers most of the interior.
- The lesser curvature of the PIG is longer and has less of an angle than the HORSE. Attached to the lesser curvature is the lesser omentum, and attached to the greater curvature is the greater omentum. The space formed between the two layers of the greater omentum is the omental bursa.
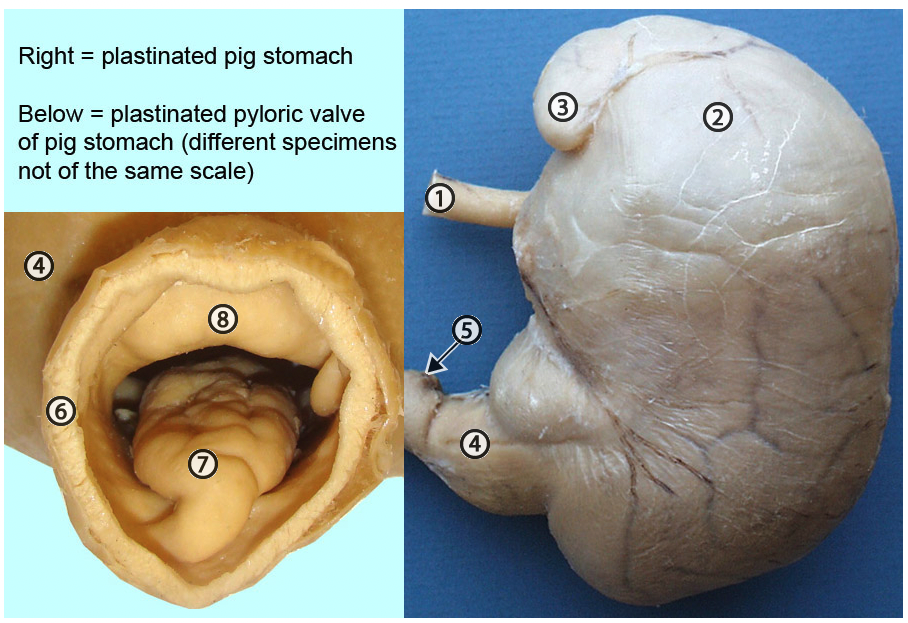
Pig stomach specimens. 1, esophagus; 2, fundus; 3, gastric diverticulum; 4, pyloric region; 5, duodenum; 6, cut edge of duodenum; 7, torus pyloricus; 8, pyloric sphincter. Since the sphincter is incomplete, the torus fills the break in the sphincter and also protrudes into the lumen of the pyloric canal. Therefore, 7 and 8 work together to close the pyloric canal. http://vanat.cvm.umn.edu/ungDissect/Lab14/Img14-17.html
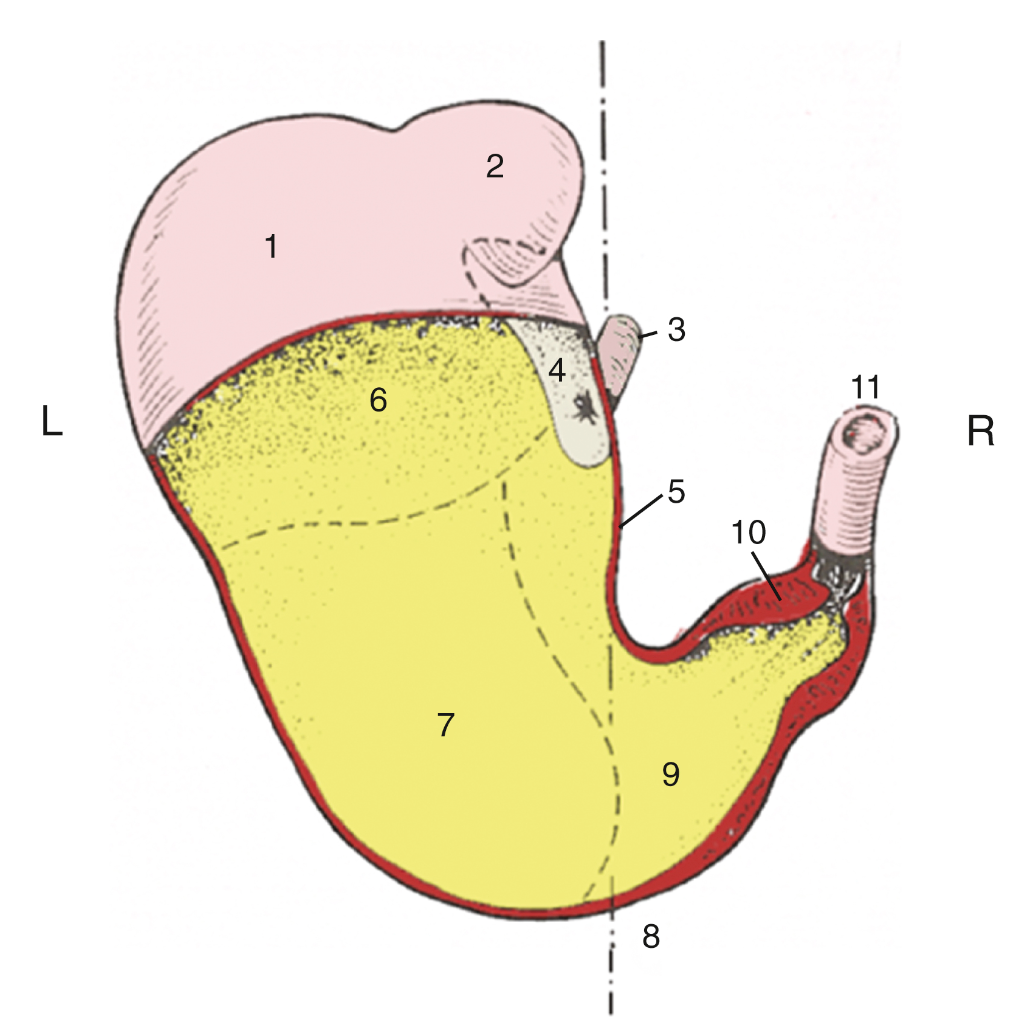
FIG. 34.8 Stomach partially opened, caudoventral view, semischematic. 1, Fundus; 2, gastric diverticulum; 3, esophagus; 4, nonglandular mucosa; 5, lesser curvature; 6, cardiac gland region; 7, region of proper gastric glands; 8, approximate position of median plane; 9, pyloric gland region; 10, torus pyloricus; 11, duodenum. TVA
Objective
A6.4 Identify and describe the anatomical features of the small and large intestines among ungulates (equine, bovine, porcine, camelid); describe the functional significance of the extensive ascending colon and summarize the normal flow of ingesta through the GI tract in the equine.
- The small intestines include the duodenum, jejunum, and ileum.
- The large intestines include the ascending colon, cecum, transverse colon, and descending colon.
BOVINE/RUMINANT = foregut fermenter, herbivore; More on RUMINANT GI tracts in the next application.
- The largest modification in ruminants is the stomach, which has four compartments including a large rumen.
- There is also a modification to the ascending colon called the spiral colon (in the shape of a flattened spiral, keeping the ascending colon compact). There is a proximal loop leading into the first half of the spiral (centripetal loops or “center seeking”), a central flexure, and then a second half of the spiral leading out (centrifugal loops or “center fleeing”) to the distal loop.
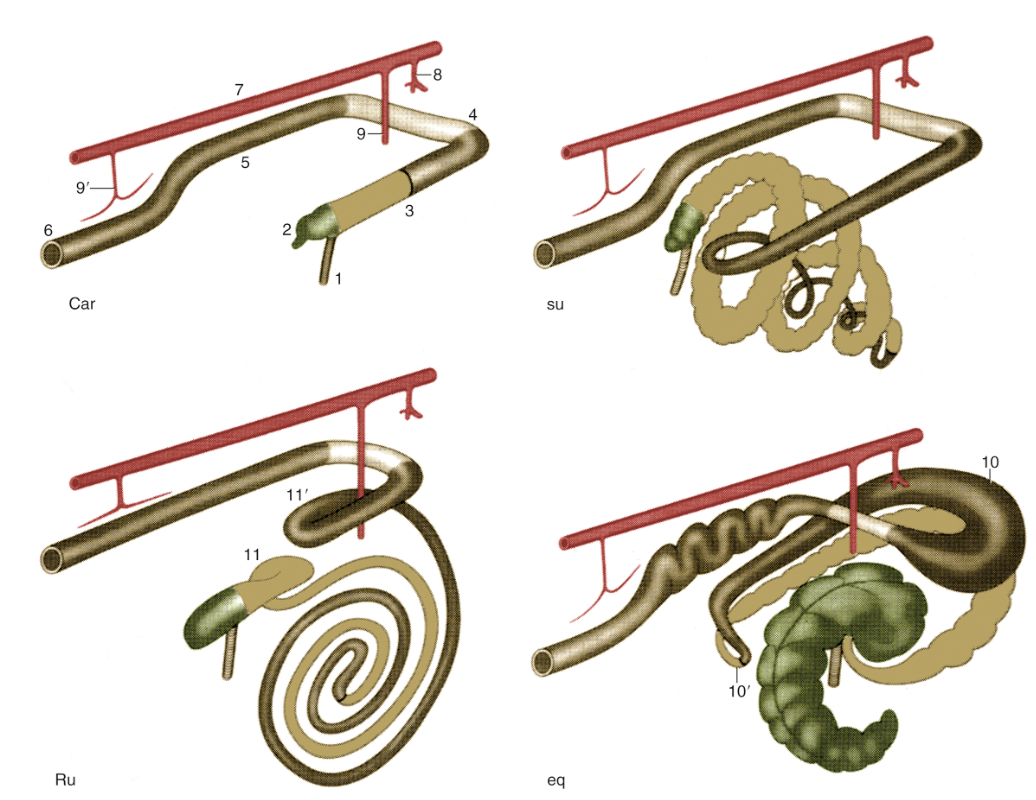
FIG. 3.45 Schematic drawing of the large intestine of the domestic mammals: carnivores (Car), the pig (su), ruminants (Ru), and the horse (eq). Cranial is to the upper right. 1, Ileum; 2, cecum; 3, ascending colon; 4, transverse colon; 5, descending colon; 6, rectum and anus; 7, aorta; 8, celiac artery; 9 and 9′, cranial and caudal mesenteric arteries; 10 and 10′, dorsal diaphragmatic and pelvic flexures of ascending colon; 11 and 11′, proximal and distal loops of ascending colon. TVA
PORCINE/SWINE/PIG = hindgut fermenter, omnivore
- The PIG GI tract is very similar to carnivores. There is a relatively straight duodenum from the stomach to the more convoluted jejunum. The ileum straightens as it enters the ascending colon.
- The PIG has a prominent feature near the junction of the ileum, cecum, and colon, called the ileal papilla. The ileum enters into the cecum via this distinctive projection (Figure 10B-6/4). An ileal papilla is well developed in the PIG but is not seen as prominently in other domestic animals.

Figure 10B-6 (Above) Dry pig cecum with a window cut to expose the ileal papilla (4). 1, apex of cecum; 2, initial part of colon; 3, ileum; 4, ileal papilla. (The ileal papilla opens into the colon and marks the initial part of the colon.)
- Pigs have a spiral colon with centripetal and centrifugal loops and a central flexure, but the centrifugal loops are narrower in diameter. There are no proximal and distal loops, and the spiral colon is in a cone configuration (bound together by mesentery) and is not flat. (see Fig. 3.45 above, and image below)
- The cecum and centripetal loop are marked by two longitudinal smooth muscle bands that pull the wall into pleats known as sacculations.

Figure above – porcine GI tract; labeled structures: esophagus, gastric diverticulum, fundus, stomach, torus pyloricus, duodenum, caudal duodenal flexure, jejunum, ileum, cecum, ascending colon (centripetal turns), central flexure, ascending colon (centrifugal turns), transverse colon, descending colon, rectum; cranial mesenteric a., caudal mesenteric a.
EQUINE = hindgut fermenter, herbivore (Fig. 21.12)
- From the pylorus of the stomach, there are descending and ascending portions of the duodenum. There is a highly mobile jejunum, and the ileum enters the cecum at the ileocecal orifice/ileal orifice.
- Equine have a large cecum and extensive ascending colon. This allows for a large vat to break down grasses. The cecum can become gas filled and cecal trocarization can be performed to decompress the cecum.
- The cecum, has a base, body, and apex. (The term ‘base’ may be misleading since the base of the cecum is the most dorsal part. It is called the base because it is the widest part).
- The cecocolic orifice leads from the base of the cecum into a large diameter right ventral colon. The right ventral colon curves at the diaphragm via a ventral diaphragmatic flexure (aka sternal flexure) and continues as the left ventral colon.
- On the left side, the left ventral colon narrows and transitions to the left dorsal colon at the pelvic flexure. The left dorsal colon curves at the diaphragm via a dorsal diaphragmatic flexure (aka diaphragmatic flexure) and continues as the right dorsal colon. The colon narrows into the short transverse colon and then a longer and narrower descending (aka small) colon. The dorsal and ventral colon look like two horseshoes stacked on top of each other.
- Large intestine bands and sacculations are seen in the PIG, HORSE, and RABBIT, and human.
- The cecum has bands and sacculations.
- The characteristics of the ventral colon are bands and sacculations (like little pouches, aka haustra) that are very prominent. The bands are smooth muscles (i.e., teniae) in the wall of the colon that contract and cause sacculations. The dorsal colon is relatively smooth along its wall, even though it still has smooth muscle bands.
- The descending/small colon has small bands and sacculations. The descending colon has two bands, mesenteric and antimesenteric: the antimesenteric band (opposite the mesentery edge) is easy to see but the mesenteric band (along the mesenteric edge) is hidden in the attachment of the mesentery to the gut.
- One feature that helps identify the small intestines from the descending/small colon is the small intestines do not have bands and sacculations.
- Functional significance of ascending colon in equine: the cecum and ascending colon are the seat of the microbial fermentation that makes the cellulose constituents of the diet available, which is comparable to the chambers of the ruminant stomach. The large intestine is so voluminous that it is almost always encountered immediately when the abdomen is opened.
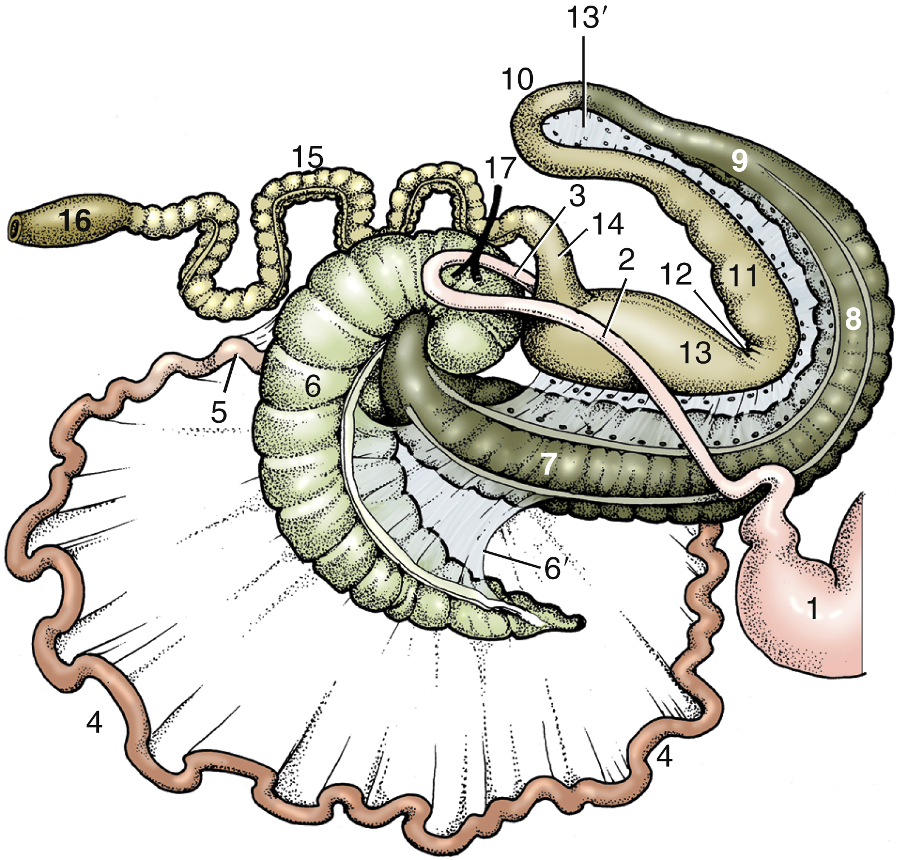
FIG. 21.12 The equine intestinal tract seen from the right (schematic). The caudal flexure of the duodenum and the cranial mesenteric artery (17) have been displaced to the right of the animal to lie over the base of the cecum. 1, Stomach; 2 and 3, descending and ascending duodenum, respectively; 4, jejunum; 5, ileum; 6, cecum; 6′, cecocolic fold; 7, right ventral colon; 8, ventral diaphragmatic flexure; 9, left ventral colon; 10, pelvic flexure; 11, left dorsal colon; 12, dorsal diaphragmatic flexure; 13, right dorsal colon; 13′, ascending mesocolon; 14, transverse colon; 15, descending (small) colon; 16, rectum; 17, cranial mesenteric artery. TVA
Normal flow of ingesta through the equine GI tract
esophagus > stomach (cardia, fundus, body, pylorus) > duodenum (descending > caudal duodenal flexure/loop > ascending) > jejunum > ileum > ileocecal/ileal orifice > cecum (base, body, apex) > cecocolic orifice > ascending colon (right ventral colon > ventral diaphragmatic flexure > left ventral colon > pelvic flexure > left dorsal colon > dorsal diaphragmatic flexure > right dorsal colon) > transverse colon > descending/small colon > rectum > anus
Objective
A6.5 Define and describe the related anatomical structures associated with bowel entrapment and impaction.
Things that lead to “colic” in equine… (colic has become a broad term for a variety of conditions that cause horses to experience abdominal pain)
Bowel entrapment: a piece of bowel gets stuck or trapped (aka incarcerated) within a certain region. Common bowel entrapment locations (see images below):
- Epiploic foramen: small intestines (e.g., distal jejunum and ileum) can get pushed into this small hole and get trapped. Usually horses older than 7 years are more frequently affected by epiploic foramen entrapment.
- Nephrosplenic space: part of the left colon can get caught over the nephrosplenic ligament and in the nephrosplenic space.
Exposure of equine abdominal viscera on the right side. 1, quadrate lobe of liver; 2, right lobe of liver; 3, caudate lobe of liver; asterisk, epiploic foramen; 4, caudal duodenal flexure; 5, base of cecum; 6, right dorsal colon. http://vanat.cvm.umn.edu/ungDissect/Lab13/Img13-8.html
View of left equine abdomen, manual reflection of the base of the spleen (1) to expose the nephrosplenic ligament (2) and the left kidney (3). 4, last rib; 5, small colon; 6, small intestine; 7, left ventral colon. http://vanat.cvm.umn.edu/ungDissect/Lab13/Img13-6.html
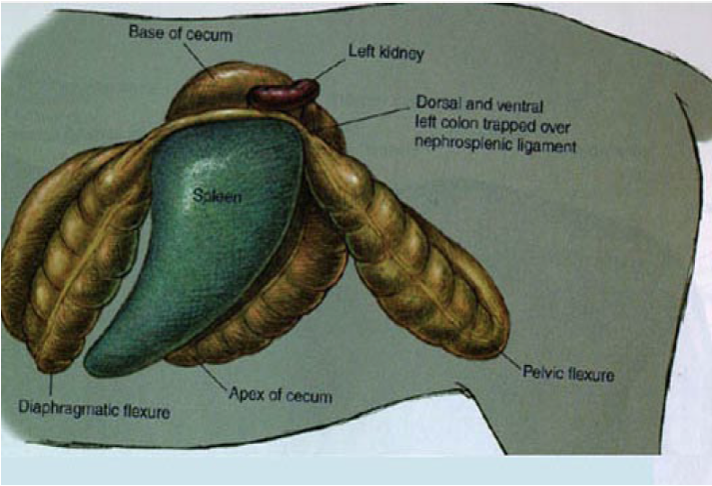
Figure (above) shows entrapment of dorsal and ventral left colon in the nephrosplenic space, created by the nephrosplenic ligament; structures in image: base of cecum, left kidney, left dorsal colon, left ventral colon, dorsal diaphragmatic flexure, apex of cecum, pelvic flexure.
Impaction: the lodging of feces in a body passageway or cavity. Impaction is common in EQUINE, as these are regions where there are diameter changes, curves, junctions, or changes in function of the GI tract segments. (Supplemental Clinical LAS Impactions – Cecal, Colon and Small Colon; LAS Impactions – stomach and small intestine)
Common impaction sites (see image below):
- Ileum, ileocecal orifice: the smaller diameter ileum enters the cecum (at the ileocecal orifice).
- Cecum, cecocolic orifice: the cecum has a large lumen and empties into a narrow cecocolic orifice in the right ventral colon (RVC).
- Pelvic flexure: this is a curve between the left ventral colon (LVC) and left dorsal colon (LDC) and is a site where the GI tract is more narrow.
- Transverse colon, descending/small colon: the right dorsal colon (RDC) is large in diameter and continues into a smaller diameter transverse colon. The transverse colon is short and quickly transitions to descending/small colon.
- Risk factors: dehydration, parasites, sandy soil, insufficient roughage or poor food quality, certain medications, confinement, and/or reduced GI motility can all be risk factors for impactions.
- (Supplemental information on Impaction: the underlying reason for impaction of the cecum is unknown, although it has been speculated that cecal muscular activity is abnormal in affected horses. Other predisposing factors include feed that is too coarse, diseased or poorly managed teeth, and insufficient water intake. Impactions also may develop secondary to other intestinal diseases and may be associated with prolonged hospitalization. Consequently, the fecal output of horses being treated for other abnormalities should be assessed on a routine basis. This is especially important in horses receiving NSAIDs on a daily basis.)
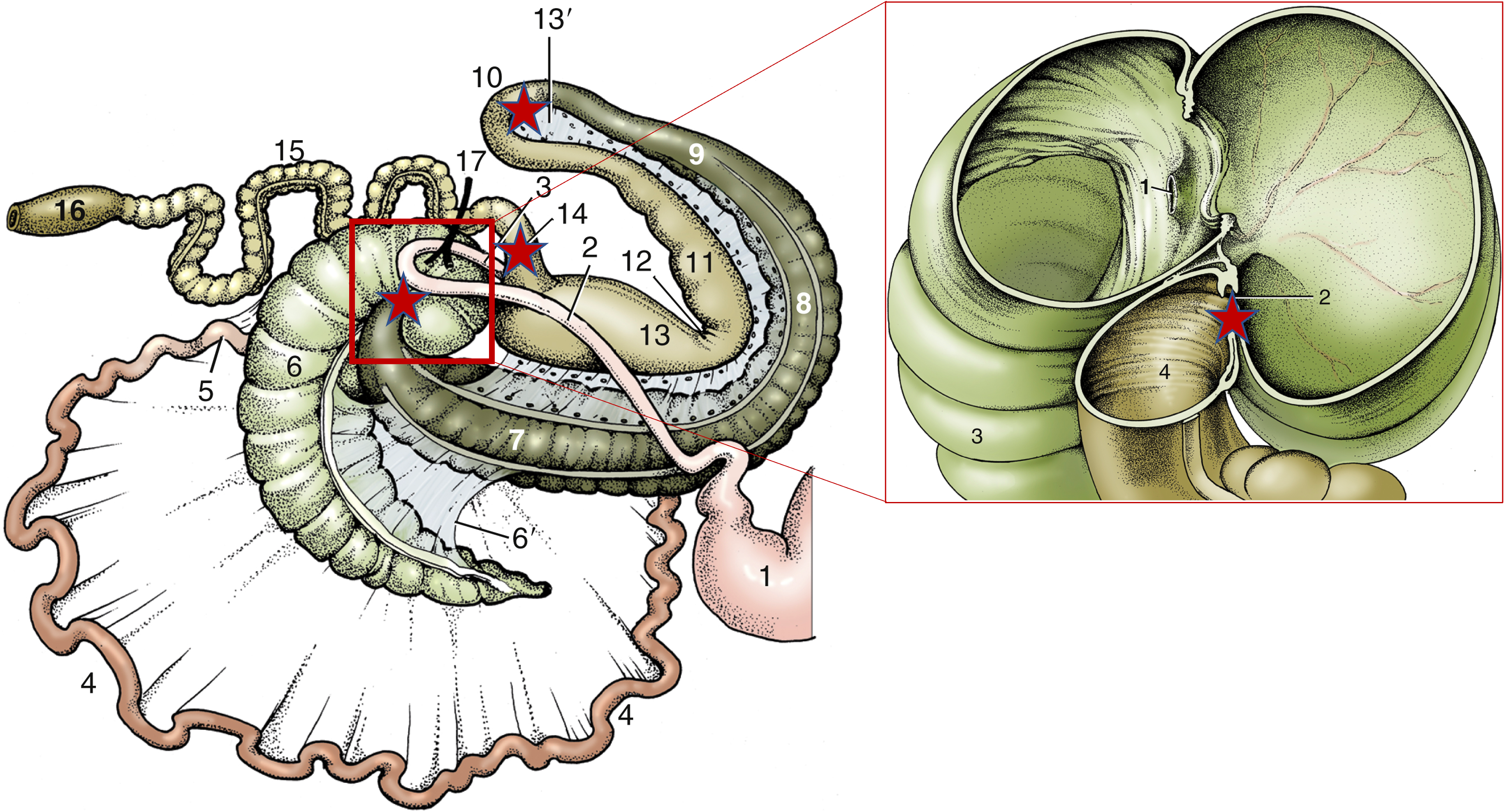
FIG. 21.12 The equine intestinal tract seen from the right (schematic on left). The caudal flexure of the duodenum and the cranial mesenteric artery (17) have been displaced to the right of the animal to lie over the base of the cecum. 1, Stomach; 2 and 3, descending and ascending duodenum, respectively; 4, jejunum; 5, ileum; 6, cecum; 6′, cecocolic fold; 7, right ventral colon; 8, ventral diaphragmatic flexure; 9, left ventral colon; 10, pelvic flexure; 11, left dorsal colon; 12, dorsal diaphragmatic flexure; 13, right dorsal colon; 13′, ascending mesocolon; 14, transverse colon; 15, descending (small) colon; 16, rectum; 17, cranial mesenteric artery. TVA
FIG. 21.16 The interior of the base of the cecum, right lateral view (schematic on right). 1, Termination of ileum at ileal papilla; 2, cecocolic orifice; 3, body of cecum; 4, right ventral colon. TVA
Red stars at some possible impaction sites: pelvic flexure, transverse colon, cecocolic orifice.
**Supplemental Clinical**
Some potential causes of colic: this material is directly from Merck Vet Manual (there is additional text and images on this linked page).
- Volvulus: a small-intestinal volvulus is seen when the intestine rotates on its mesenteric axis >180°. As the degree of the rotation increases, the vascular supply to the intestine is lost. Presumably because of its attachment to the cecum, the distal aspect of the volvulus is the ileum in most cases.
- Incarceration: the distal jejunum and ileum are the most common portions of the intestine that become incarcerated through the epiploic foramen. Although generally the intestine passes through the epiploic foramen from left to right, tearing the omentum in the process, it also may pass in the opposite direction to enter the omental bursa.
- Pedunculated lipomas: are suspended from the mesentery by a stalk or pedicle, which wraps around a segment of intestine, occluding the lumen of the intestine and interfering with its blood supply. The lipoma frequently forms a knot with the pedicle. Usually seen in horses > 10 yr old.
- Intussusception: invaginated segment of the GI tract becomes enveloped by an antegrade or retrograde segment of the GI tract. Most intussusceptions in horses are jejuno-jejunal, ileal-ileal, or ileocecal. The length of intestine that has become invaginated into the more distal segment of intestine may range from a few centimeters to as much as a meter. Although the precise cause of most intussusceptions remains speculative, alterations in peristalsis due to enteritis, surgical trauma, parasite damage, anthelmintics, and Anoplocephala perfoliata infection have been suggested. Horses < 3 yr old are affected most commonly.
**Supplemental Information on Rabbit Viscera: (you may see rabbit viscera in the anatomy lab; an understanding of rabbit anatomy is gaining in importance – e.g., GI surgery, GI radiographs, GI stasis)**
- Rabbit Cecum:
- Similar to the EQUINE, the rabbit has a very large cecum (the largest of all animals relative to body size) with prominent sacculations, however the bands are more subtle.
- The sacculus rotundus is a round dilatation of the cecum marking the ileocecal junction.
- The cecum has a long vermiform (worm-like) appendage on the apical (apex) end which resembles the HUMAN appendix, and is referred to as the appendix of the cecum. Massive amounts of lymphoid tissue reside within its walls.
- Rabbit Colon:
- The colon is only about half the diameter of the cecum, and is divided into a sacculated proximal colon (with well-defined bands) and a non-sacculated distal colon.
- Rabbits produce dry hard feces and soft mucoid feces.
- The soft mucoid feces are the so-called ‘night feces’, or cecotrophs, that come from the cecum and pass through the colon with little water absorption. Goblet cells in the colon add mucous to the cecotrophs.
- In contrast, water absorption in the colon is responsible for production of dry feces.
- Coprophagy, the consumption of feces/stools, is abnormal in many species but normal in rabbits. The cecotrophs are eaten as they pass through the anus and are swallowed whole without chewing. The mucous coating prevents digestion while the cecotrophs ferment in the fundus of the stomach.
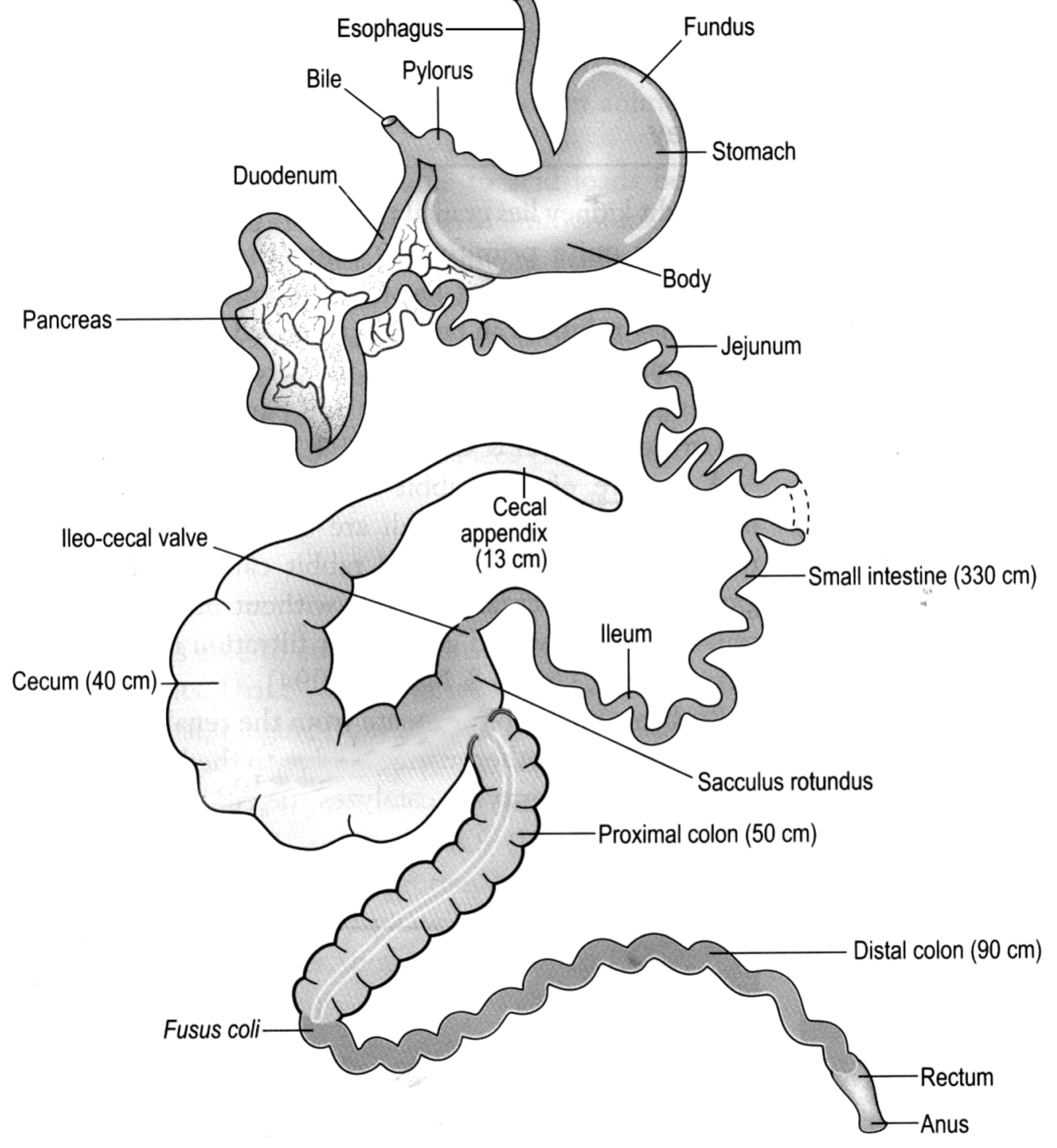
Fig. 10B-7: Rabbit gastrointestinal tract, a schematic illustration