
1 Thoracic Limb
Revised Spring 2024 by T. Clark
Additional Resources for this Chapter:
- Valuable Supplemental Large Animal Surgery (LAS) course eBook links (starting with Equine Lameness and going through Swine, Small Ruminant, and Poultry Lameness): Carpal Joint Injuries; LAS Physeal disorders; LAS Gait Abnormalities; LAS Nerve damage
- Veterinary Gross Anatomy Ungulate Dissection (Limb Dissection Labs 1-7)
- Associated Video Links:
- Thoracic Limb Bones (7 videos, 20:28)
Objective
A1.1 Describe and differentiate regions and bones of the (proximal) thoracic limb (from scapula to carpus) by using correct directional/regional terminology.
Note: The terms thoracic limb and forelimb may be used interchangeably.
Directional Terms (repeat from Small Animal Anatomy and Vet Basics)
- Dorsal/ventral, cranial/caudal, medial/lateral, proximal/distal, dorsal/palmar, superficial/deep
Regions of the Thoracic Limb: (repeat from Small Animal Anatomy and Vet Basics)
- Shoulder: scapula
- Brachium (arm): humerus
- Antebrachium (forearm): radius, ulna
- Manus (forepaw): carpus, metacarpal bones, digit(s) made up of phalanges and sesamoid bones
Note: The distal limb (distal to carpus and tarsus) in the ungulate is longer than the same region in the carnivore. “Ungulate” positioning has lengthened the limb and this allows them to be faster (see image below, left is ungulate forelimb bones scaled to fit canine forelimb bones).

Superficial Structures: (There are labeled images in the Appendix/Back Matter with some of these structures as well.)
- Chestnut (eq) – A keratinized structure on the medial side of the thoracic limb, proximal to the carpus. There is also a chestnut on the medial side of the pelvic limb, distal to the tarsus. These are thought to be similar to the
metacarpal/metatarsalcarpal/tarsal pads of dogs and cats. - Ergot (eq) – keratinized growth on the palmar (and plantar) surface of the fetlock.
- Coronet (p) – the skin to hoof (or skin to claw) transition; the ‘crown’ of the hoof. Deep, and distal, to the coronet is a band of dermal tissue (the coronary band). Some may confuse and interchange the terms coronet and coronary band.
- Dewclaws (bov) – underdeveloped digits 2 and 5 (palmar and plantar surfaces).
Bones:
Scapula (Fig. 1-1 and TVA 591)
- The scapular cartilage is well developed in ungulates, small in the dog, and absent in humans. In some cases, the cartilage may ossify. Observe skeletal models for remnants of this cartilage.
- The HORSE and PIG lack an acromion on the distal end of the spine of the scapula but have a tuberosity in the middle of the spine, the tuber spinae. (The absence of the acromion leads to a variation in muscles which normally attach here, (e.g., omotransversarius [bov] and part of the the deltoideus). The spine of the scapula is an often used palpable landmark.
- The OX has an acromion on the distal end of the spine of the scapula, but not a tuber spinae.
- Note the supraglenoid tubercle on the distal end of the scapula. (This tubercle is the region of origin for the biceps brachii m. tendon.) In EQUINE, the supraglenoid tubercle can fracture.
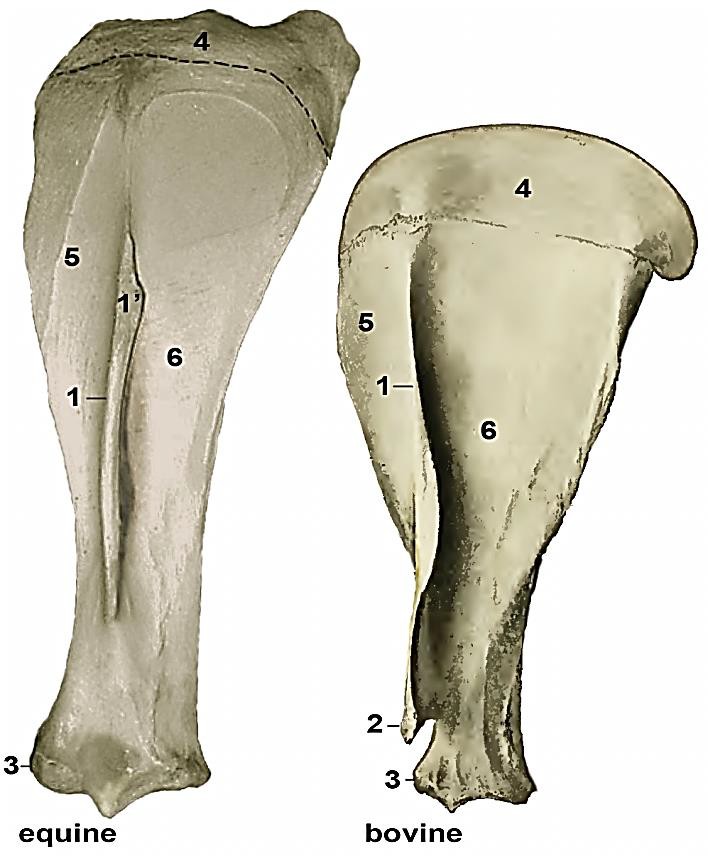
Figure 1-1 Left scapula, lateral view. 1, spine; 1′, tuber spinae (horse only); 2, acromion (ox only); 3, supraglenoid tubercle; 4, dorsal scapular cartilage; 5, supraspinous fossa; 6, infraspinous fossa. (Modified from Sisson and Grossman, 1930)
Humerus (Fig. 1-2)
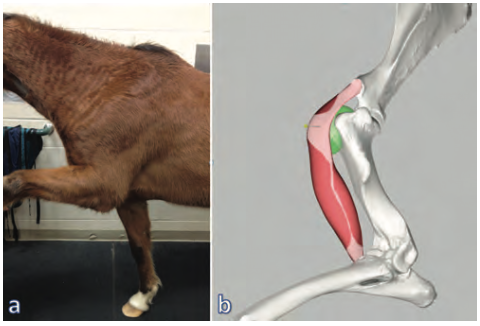
- The intertubercular (aka bicipital) groove of the HORSE is divided by an intermediate ridge that functions to stabilize the biceps brachii tendon (aka bicipital tendon) as it passes through the groove. This ridge is only found in EQUIDS and CAMELIDS. The bicipital groove can be used as a landmark on ultrasound, and the bicipital bursa (see green bursa in image below) can become inflamed.
- On either side of the intertubercular groove there are the greater and lesser tubercles located laterally and medially, respectively. The ascending deep pectoral m. inserts on these tubercles.
- Identify the deltoid tuberosity on the lateral side of the shaft of the humerus, the point of attachment for the deltoideus m.
- Note the deep brachialis groove that contains the brachialis m.
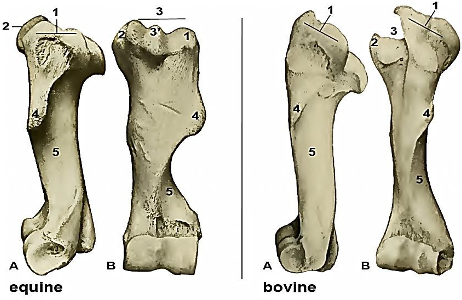
Figure 1-2 Left humerus. A, lateral view; B, cranial view. 1, greater tubercle; 2, lesser tubercle; 3, intertubercular groove; 3′, intermediate ridge (horse only); 4, deltoid tuberosity; 5, brachialis groove. (Modified from Sisson and Grossman, 1930)
Radius and Ulna (Figs.1-3, 1-4)
- The radius is the primary weight bearing bone in the antebrachium.
- The distal end of the radius presents grooves for several extensor tendons (extensor carpi obliquus [abductor digiti I longus in the DOG], extensor carpi radialis, common digital extensor, and lateral digital extensor mm).
- In the adult HORSE and OX the ulna is fused with the radius and is quite reduced in size (i.e., vestigial) resulting in an inability to pronate and supinate the limb.
- Proximally, note an area of incomplete fusion between the radius and ulna, the interosseous space. Either the common interosseous a. (EQUINE) or cranial interosseous a. (OX) travels through this space to reach the antebrachial muscles.
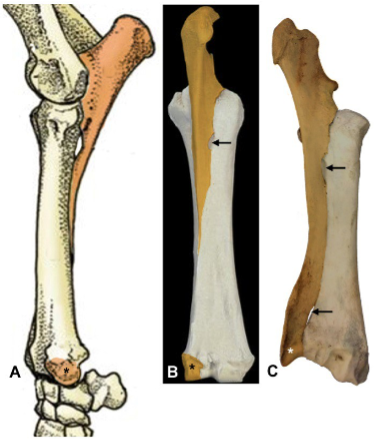
Figure 1-3 Left radius and ulna of the horse, (A) lateral view and (B) caudal view and bovine, (C) caudomedial view. Approximate regions belonging to the ulna have been shaded brown. Arrows, interosseous spaces; *, lateral styloid process.
- In the OX, note the distinct lateral styloid process of the ulna; in the HORSE this process will be less distinct but still identifiable. In the adult horse, the distally located lateral styloid process of the ulna is completely fused to the radius; however, separation (not fracture) of this process is a normal variation seen in some horses (Fig. 1-4).
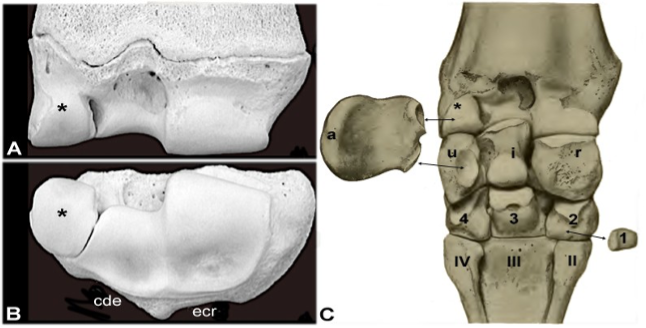
Figure 1-4 (A) Caudal view and (B) articular surface of the left distal radius of a yearling horse. Grooves on cranial surface of distal radius for the tendons of common digital extensor (cde) and extensor carpi radialis (ecr); *, lateral styloid process (remnant of distal ulna); (Image source: V. Cox U of MN). (C) Palmar view of the left carpus of a mature horse. Carpal bones, proximal row: a, accessory; u, ulnar; i, intermediate; r, radial. Carpal bones, distal row, Arabic numbers (1,2,3,4) correspond to bone identification; Metacarpal bones are labeled with Roman numerals (II, III, IV); *, Lateral styloid process. Note: In mature horses the lateral styloid process fused to the radius proper. (Modified from Sisson and Grossman, 1930, Fig. 73).
- In the PIG the radius and ulna remain as two complete bones.
- In PRIMATES the radius and ulna are separate bones, very mobile, and allow for supination and pronation. The interosseous membrane is present and forms between the radius and ulna.
- In CARNIVORES the radius and ulna are typically separate bones and but there is more limited movement (i.e., supination and pronation) of the radius and ulna. Cats tend to have more movement than dogs. An interosseous ligament is present between the radius and ulna, and interosseous vessels travel through and into this ligament and space.
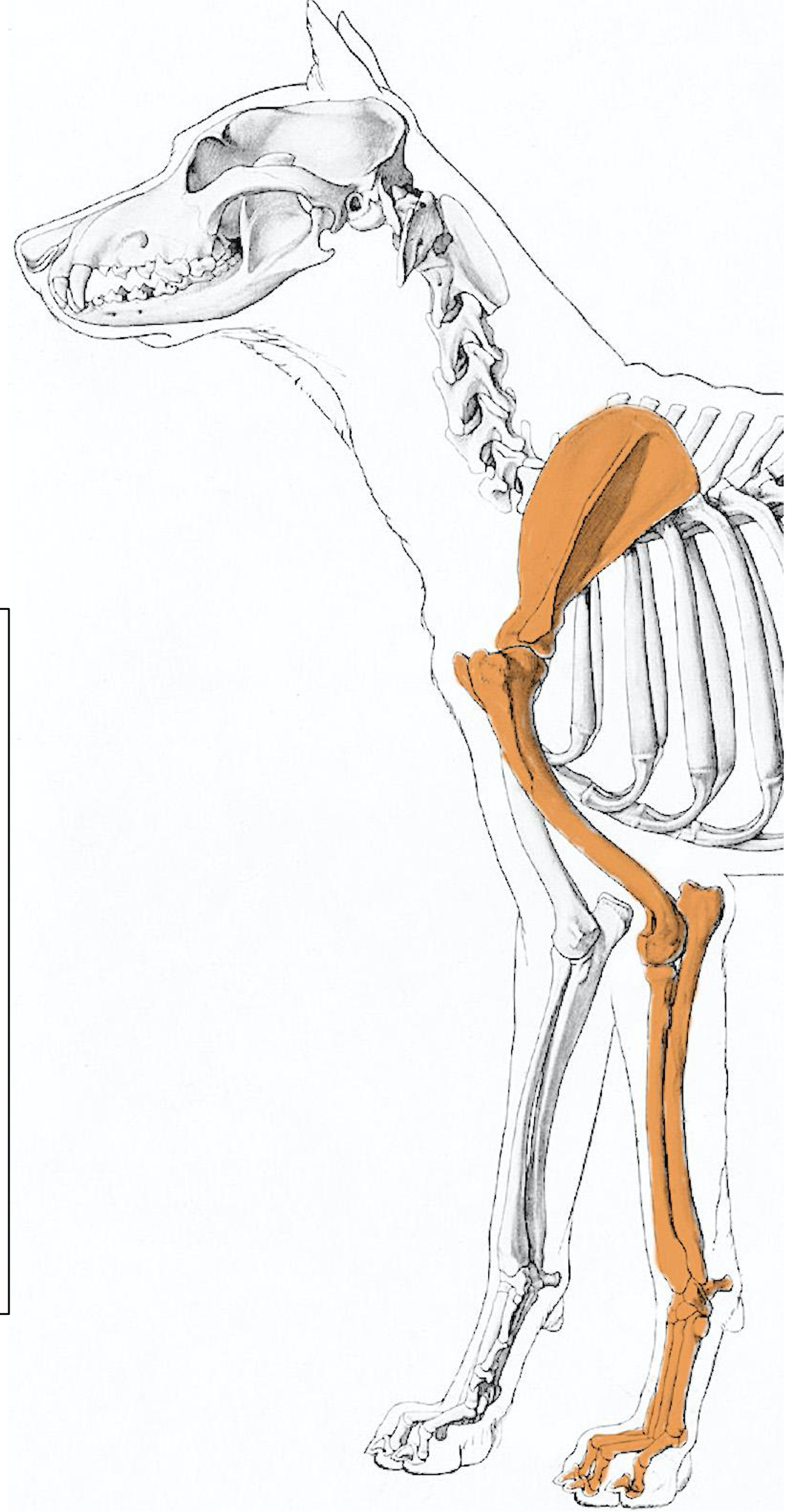
Figure Above: Carnivore (dog) thoracic limb and arrangement of radius and ulna.
Carpal bones (Figs. 1-5, 1-6)
- The HORSE has 7 (or 8) carpal bones and the OX has 6.
- In the EQUINE, BOVINE, and PORCINE the first row of carpals are separate bones, from medial to lateral: radial carpal bone, intermediate carpal bone, ulnar carpal bone, and accessory carpal bone.
- The accessory carpal bone is convex laterally and projects caudomedially from its lateral articulation. It forms the lateral wall of the carpal canal and is a ‘lever-like’ bone.
- Since the accessory bone is on the lateral aspect of a normal carpus, this can help you identify a left carpus from a right carpus.
- The distal row of carpal bones is comprised of two to four (numbered) bones.
- In the HORSE, C1 is often absent (radiographically present in 15% – 20% of equine carpi). C1 and C2 are fused or partially fused, therefore the distal row usually consists of second (C2), third (C3), and fourth (C4) carpal bones, for a total 7 carpal bones (or 8, if C1 is present).
- In EQUINE, the 2nd carpal bone (C2) is directly supported by the 2nd metacarpal bone (Mc2), while the 4th carpal bone (C4) straddles the 3rd and 4th metacarpals (Mc3 and Mc4).
- In the OX, C1 is absent, the second (C2) and third (C3) carpal bones are fused, and the fourth carpal bone (C4) is present, hence there are a total of 6 carpal bones in the bovine.
- In the PIG, C1, C2, C3, and C4 are all present as separate bones, which makes a total of 8 carpal bones in the pig.
- In the HORSE, C1 is often absent (radiographically present in 15% – 20% of equine carpi). C1 and C2 are fused or partially fused, therefore the distal row usually consists of second (C2), third (C3), and fourth (C4) carpal bones, for a total 7 carpal bones (or 8, if C1 is present).
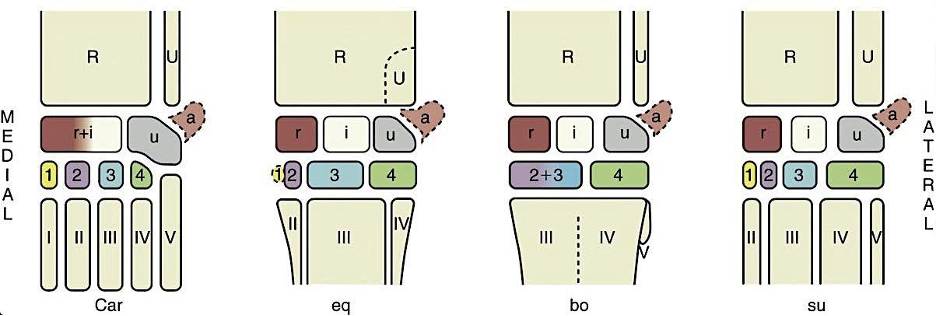
Figure 1-5 Comparative left carpal anatomy (schematic): car, carnivore; eq, horse; bo, cattle; and su, pig. Roman numerals (I-V) identify the metacarpal bones; Arabic numerals, the distal carpal bones. R, Radius; U, ulna; a, accessory carpal bone; i, intermediate carpal bone; r, radial carpal bone; u, ulnar carpal bone. (TVA)
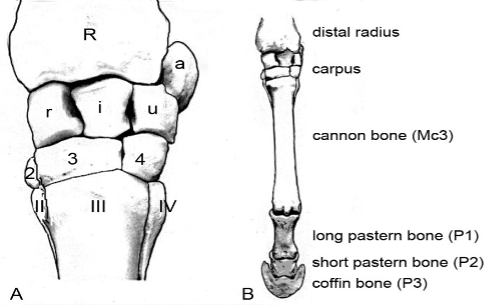
Figure 1-6 Equine, left forelimb, dorsal view. A, carpus; B, carpus, metacarpus and digit.
- Clinical Notes: in the HORSE (especially racehorses), common forelimb problem areas involve the carpus and more distally (especially the foot), less so in RUMINANT feet. Non-racehorses have arthritis and related disorders. Supplemental Clinical Information LAS Carpal Joint Injuries (LAS eBook)
- Chip fractures: The major problem in the carpal joint is chip fractures; the result being small pieces of bone that must be removed from the joint through surgery. When reading carpal radiographs, the edges of the various component bones appear superimposed, so carpal chips are obscured by much larger bones. To find carpal chips, oblique and flexed lateral views are needed to position the chip in a tangential position where it is not superimposed on a larger bone. Reading different radiographic views of the carpus requires good knowledge of the shape of individual carpal bones, their articulations with adjacent bones, and normal variations (e.g., 15-20% of horses have the C1 carpal bone).
- Slab fracture of C3: alignment of the metacarpal tuberosity of the 3rd metacarpal (Mc3 aka cannon bone) with C3 during overextension can lead to a “slab fracture” of C3 (see image below).

Figure Above: Radiograph of slab fracture of C3 (white arrow); carpus in flexion.
- In the next application the metacarpals, proximal and distal sesamoids, and phalanges are discussed.
- Clinical Notes: Most, but not all, long bones have both a proximal and distal physis. Growth of the long bone occurs in the physis as most of the cells in the physis are cartilage. Physeal growth also adds to the width of the bone. Physitis, or inflammation of the physis, can occur due to excessive trauma on a normal physis or to normal trauma on an abnormal physis. Causes include rapid growth due to genetics and/or diet, excessive exercise, uneven weight due to an angular limb deformity (ALD), or abnormal cartilage. If the cause is exercise or growth, the physitis is usually symmetrical. If the physitis is asymmetrical, it is likely ALDs. (Supplemental Clinical LAS Physeal disorders)
Objective
A1.2 Identify and describe the joints, joint angles, joint actions, and muscle groups of the (proximal) thoracic limb.
Joints of the Proximal Forelimb
- Clinical Notes: joint pouches are extensions of the synovial capsule and cavity past the joint surface. In more mobile joints these pouches can be more expansive/extensive. When you “tap a joint” (i.e., aspirate) you will not always remove fluid right at the bony union of a joint, but rather near the extension of these synovial cavities. These pouches may also bulge outwards and can visibly be seen due to inflammation. Additionally, anesthesia can be injected in and near the joint capsules.
- Shoulder joint (aka glenohumeral joint, scapulo-humeral joint): the humeral head articulates with the glenoid cavity of the scapula. The tendon of the infraspinatus m. acts as a lateral collateral ligament with assistance from the supraspinatus m. The tendon of the subscapularis m. acts as a medial collateral ligament. The shoulder joint has no other collateral ligaments.
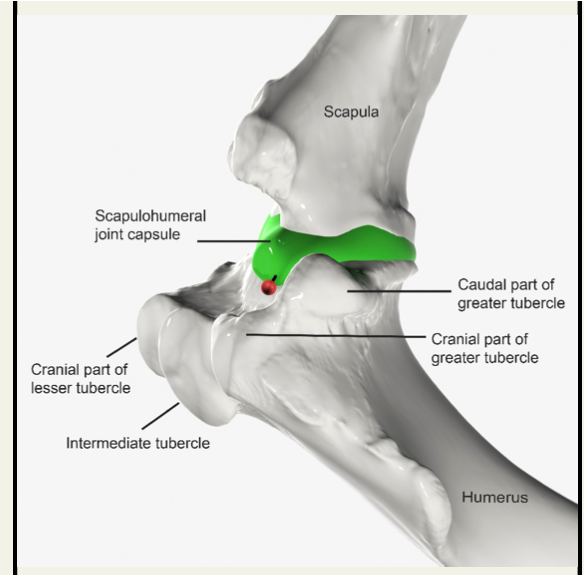
Fig 2-2: Left Forelimb. Craniolateral View of the Shoulder Joint (joint capsule/pouch in green). Approach to the shoulder joint capsule: The shoulder joint can be injected cranial to the broad tendon of the infraspinatus muscle, slightly above the caudal part of the greater tubercle. The needle is inserted between the palpable cranial and caudal parts of the greater tubercle. The needle is directed caudally, but parallel to the ground, to avoid puncturing the bicipital bursa which lies cranially. The bicipital (intertubercular) bursa is located under the tendon of origin of the biceps brachii muscle. Unlike dogs, the bursa does not communicate with the shoulder joint capsule in horses. (Equine Joint Injection and Regional Anesthesia by Moyer, Schumacher, Schumacher, 2011; image from Equine Anatomy Guide: The Forelimb; Mansour, Steiss, Wilhite)
- Elbow joint (aka cubital joint): the joint is formed by the distal end of the humerus (trochlea and capitulum) articulating with the proximal head of the radius and the trochlear notch of the ulna. The elbow joint has medial and lateral collateral ligaments.
- The carpal joints are named, from proximal to distal:
- Antebrachiocarpal (aka radiocarpal)
- Middle carpal (aka intercarpal)
- Carpometacarpal: this joint has little to no motion.
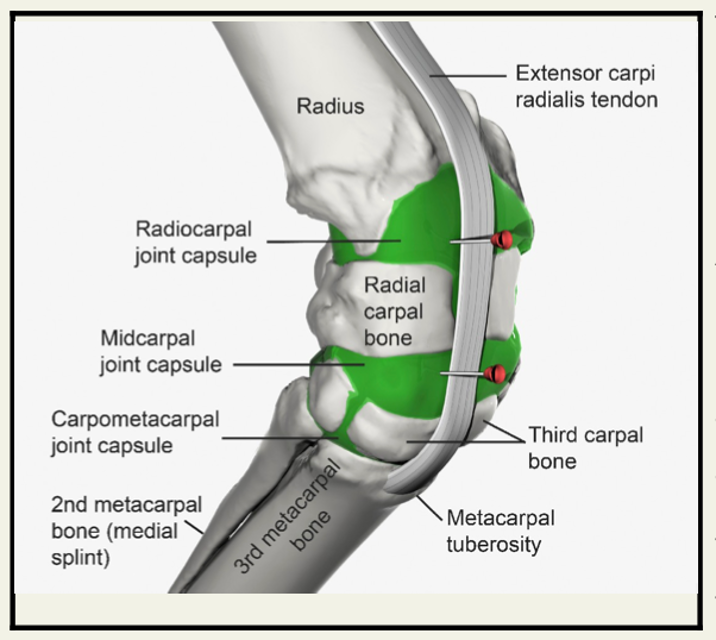
Fig 2-4: Left Forelimb. Dorsomedial View of the Carpus (joint capsule/pouch in green). A single fibrous capsule encloses 3 synovial compartments. The synovial joint capsules are: radiocarpal (antebrachiocarpal), middle (mid)carpal, and carpometacarpal. The last middle carpal and carpometacarpal compartments communicate with each other.
Approach to the carpal joint capsules: On the dorsal surface of the carpus, the broad tendon of insertion of the extensor carpi radialis muscle and the metacarpal tuberosity serve as landmarks for injection of the joint compartments of the carpus. The carpal joint capsules can be accessed easily when the limb is lifted and the carpus flexed. The radiocarpal (antebrachiocarpal) joint has a separate joint capsule. The middle carpal joint communicates with the carpometacarpal joint, which means that two injections of a drug are sufficient to treat all three compartments. With the carpus flexed, the radiocarpal joint is accessed in the palpable depression between the radius and radial carpal bone, medial to the extensor carpi radialis tendon. The middle carpal-carpometacarpal joint space is entered distal to the above site, in the depression between the radiocarpal bone and third carpal bone, medial to the extensor carpi radialis tendon. (Equine Joint Injection and Regional Anesthesia by Moyer, Schumacher, Schumacher, 2011; image from Equine Anatomy Guide: The Forelimb; Mansour, Steiss, Wilhite)
Extrinsic Muscles of the Forelimb:
- Cutaneous muscles: omobrachialis and cutaneous trunci are thin cutaneous muscles found over the proximal and lateral shoulder as well as along the thorax, respectively. They are mainly responsible for twitching the skin.
- There is a similar attachment of the forelimb to the trunk via muscles in ungulates and carnivores. Ungulates lack clavicles, which allows for more movement at the shoulder joint and increases stride length.
- Additionally, the relative muscle mass is more proximal in the limbs in the horse and dog, which is linked to their ability to run. The distal limb has very little muscle but several tendons, making the distal limbs stream-lined and provides an advantage when running at a fast speeds.
- The shoulder joint has no collateral ligaments, so a loss of muscle (i.e., atrophy) leads to subluxation and luxation at the shoulder (see Sweeney below and LAS Gait Abnormalities).
- The dorsal scapular (aka dorsoscapular) ligament offers passive support (and is a shock absorber) to the attachment of the scapula to the trunk in ungulates. The dorsal scapular ligament is better developed in the HORSE than in the BOVINE.
- Omotransversarius (bov): in the OX, the omotransversarius is separate from the brachiocephalicus m., while in the HORSE it is fused to the brachiocephalicus.
- You may find the superficial cervical lymph nodes (aka “prescaps”) deep to this muscle in the OX.
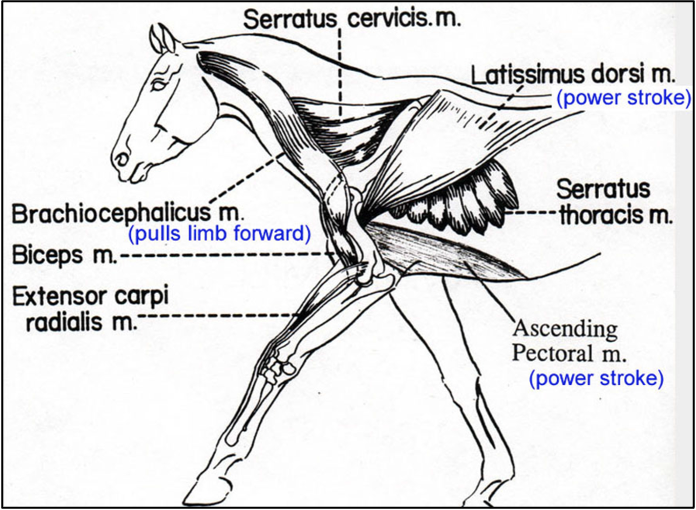
- Muscles that allow for an increased stride length in the HORSE include (image below):
- Brachiocephalicus m., which pulls the limb forward when the limb is in the air.
- Latissimus dorsi m., which pulls the trunk forward (i.e., power stroke) when the forelimb is contacting the ground.
- (Ascending or Caudal) deep pectoral m., which pulls the trunk forward (i.e., power stroke) when the forelimb is contacting the ground.
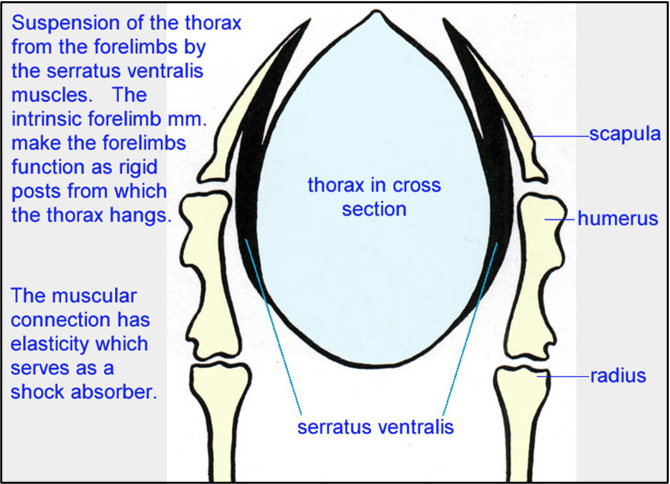
- The serratus ventralis m. (image below) in HORSES has fibrous bands that help reinforce this sling-like muscle. The serratus ventralis mm. act to suspend the thorax from the forelimbs and support the trunk. These muscles have elastic properties that allow them to function as shock absorbers. The forelimbs become rigid posts (via the intrinsic mm.) from which the thorax hangs.
- Pectoral muscles:
- Superficial (descending and transverse parts) pectoral mm. can aid in adduction of the forelimb.
- Deep pectoral mm.:
- The ascending or caudal deep pectoral m. can retract the free limb or advance the trunk when the limb is fixed.
- Subclavius or cranial deep pectoral m. (eq) is specific to the HORSE and runs along the cranial edge of the scapula and humerus.
- You may find the superficial cervical lymph nodes (aka “prescaps”) dorsal to these deep pectoral muscles in the HORSE.
- Trapezius (cervical and thoracic parts) mm. act to raise the scapula; the cervical portion can advance the forelimb; the thoracic portion can assist in swinging the forelimb caudally.
- Rhomboideus (cervical and thoracic parts) mm. act to raise and rotate the scapula.
- The latissimus dorsi m. can act to pull the trunk forward on an advanced limb (and acts as an antagonist to the brachiocephalicus m.).
- The omohyoideus (eq) is well-developed in the HORSE (and poorly developed in RUMINANTS) and is deep to the brachiocephalicus m.
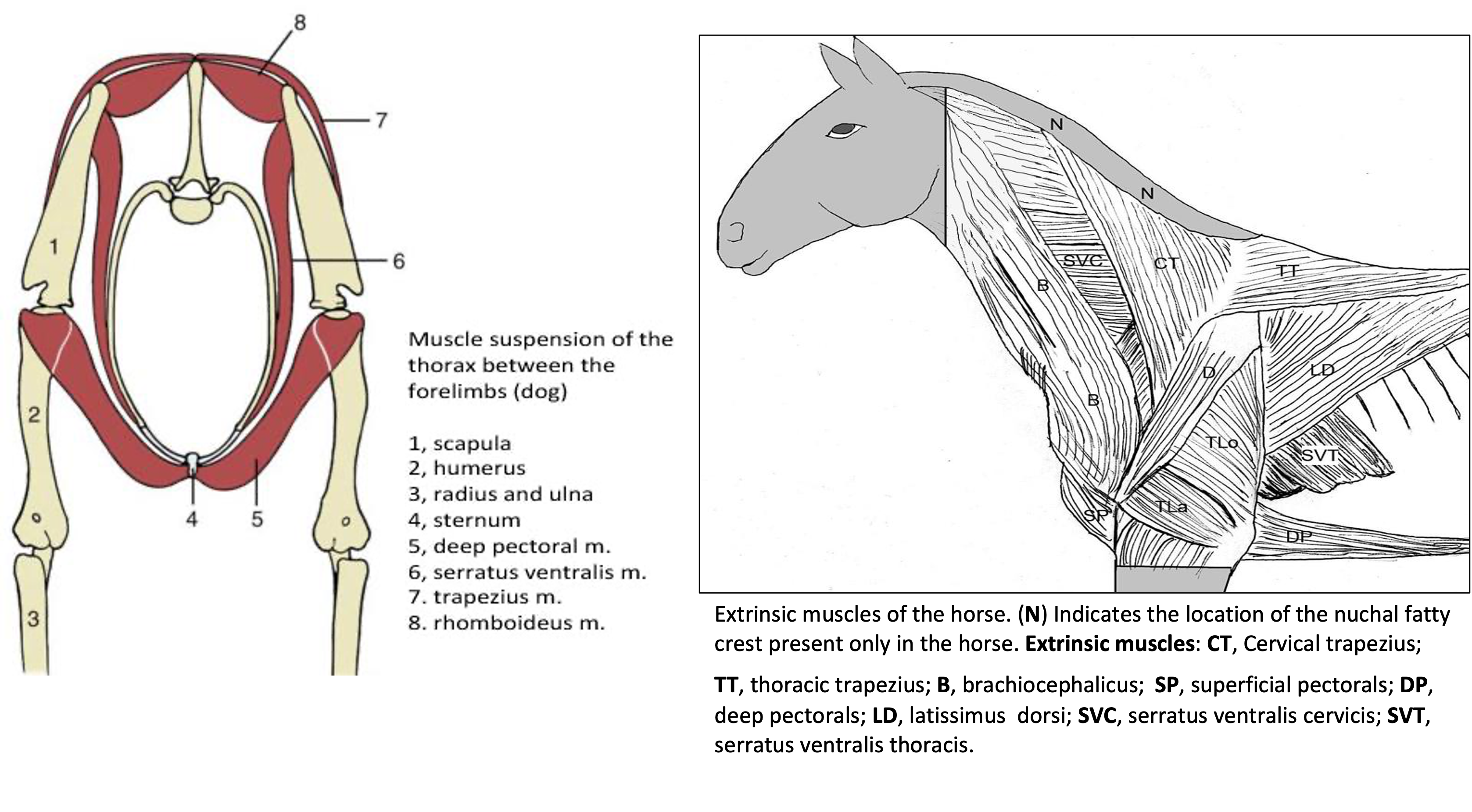
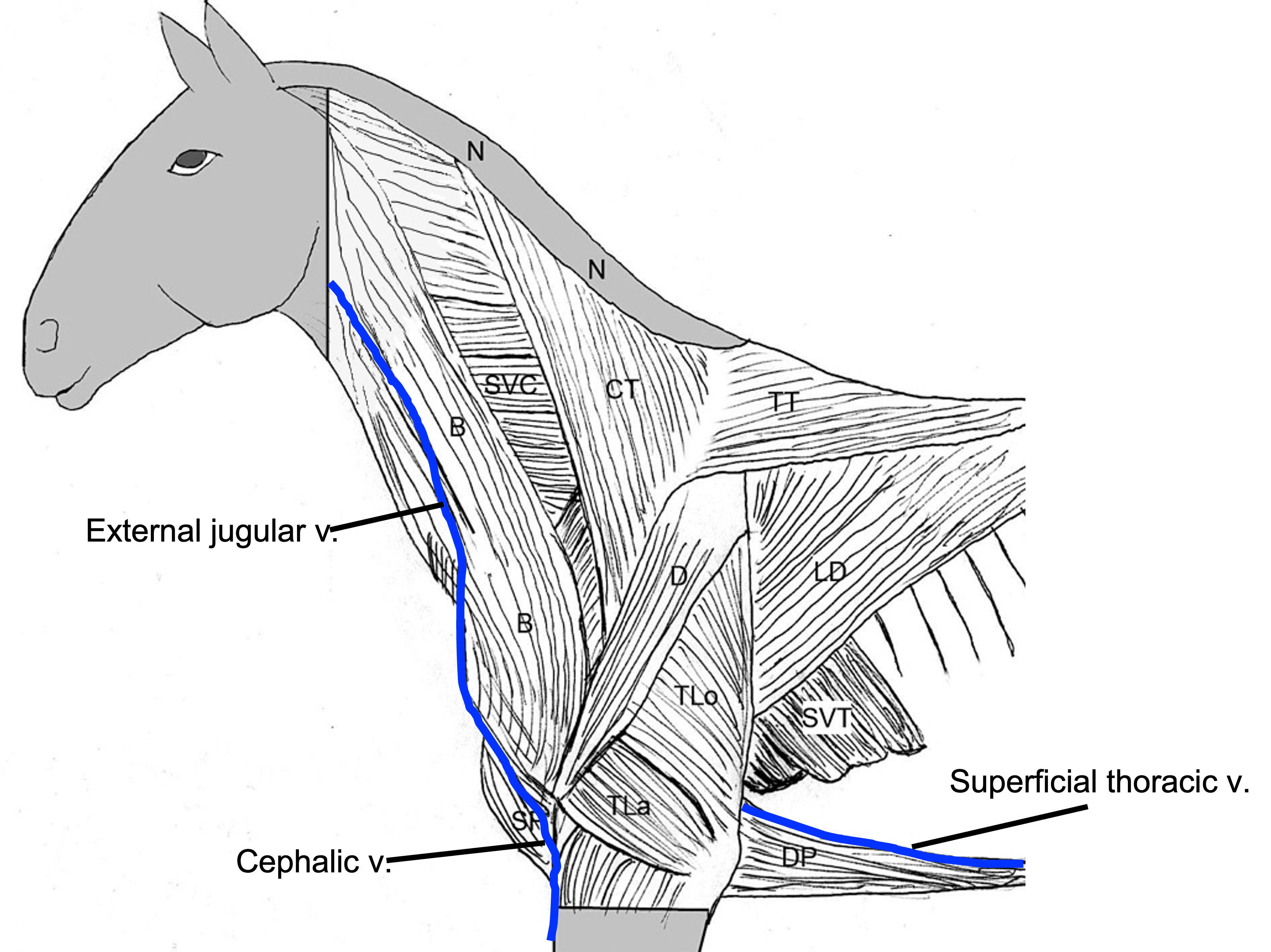
Figures above – (left) cross section of forelimbs and thoracic muscles (in the dog); labeled structures: 1, scapula; 2, humerus; 3, radius and ulna; 4, sternum; 5, deep pectoral m.; 6, serratus ventralis m.; 7, trapezius m.; 8, rhomboideus m. (right) lateral view of extrinsic muscles (in the horse); labeled structures: N, nuchal fatty crest (only in horse); CT, cervical trapezius; TT, thoracic trapezius; B, brachiocephalicus; SP, superficial pectorals; DP, deep pectorals; LD, latissimus dorsi; SVC, serratus ventralis cervicis; SVT, serratus ventralis thoracis.
Intrinsic Muscles, Joint Actions, and Muscle Groups (with Innervation) of the Proximal Forelimb:
- Subscapularis, infraspinatus, and supraspinatus mm. act to stabilize the shoulder joint (via tendons).
- Flexors of Shoulder: deltoideus m. (innervation – axillary n.)
- Deltoideus mm. act to flex the shoulder and can also abduct the forelimb.
- Extensors of Shoulder: biceps brachii m. (innervation – musculocutaneous n.)
- Biceps brachii (bicipital tendon, lacertus fibrosus [aka long tendon of the biceps brachii]) mm. act to extend the shoulder and flex the elbow.
- Flexors of Elbow: biceps brachii m., brachialis m. (innervation – musculocutaneous n.)
- Brachialis mm. act to flex the elbow.
- Extensors of Elbow: triceps brachii m. (innervation – radial n.)
- Triceps brachii (long, lateral, and medial heads) mm. act to extend the elbow.
- Tensor fasciae antebrachii (eq) mm. may be able to extend the elbow.
- Flexors of Carpus: flexor carpi ulnaris m., flexor carpi radialis m. (innervation – ulnar, median nn. respectively)
- The flexor retinaculum is a thick band of fascia extending across the palmar aspect of the carpal region (covering the carpal canal). This retinaculum binds down the flexor tendons that pass through the carpal canal.
- Extensors of Carpus: extensor carpi radials m., ulnaris lateralis (aka extensor carpi ulnaris) m. (innervation – radial n.)
- The extensor retinaculum is a band of fascia extending across the dorsal aspect of the carpal region that binds down the extensor tendons that cross the dorsal aspect of the carpus and helps keep them in place.
- Actions at Joints
Objective
A1.3 Identify and describe all components contributing to the equine suspensory apparatus and forelimb stay apparatus.
Forelimb Stay Apparatus:
- Reminder: Muscles insert onto bone via tendons (e.g., bicipital tendon). Bone to bone connections are via ligaments (e.g., collateral ligaments).
- HORSES have a special connective tissue system that allows them to conserve muscle energy while standing. In the thoracic limb this is called the passive forelimb stay apparatus, which either prevents flexion or hyperextension of specific joints to prevent collapse of the limb. The forelimb passive stay apparatus includes structures spanning from the distal scapula to the distal phalanx.
- Proximally, the biceps brachii m. attaches to the scapula via the bicipital tendon. This tendon is continuous with a central tendon running within the biceps brachii that ties distally into the connective tissue of the extensor carpi radialis m. via the lacertus fibrosus. The extensor carpi radialis m. attaches distally to the metacarpal tuberosity of the 3rd metacarpal (Mc3 aka the cannon bone).
- These structures create a long fibrous connective tissue cable running down the cranial aspect of the forelimb from distal scapula to proximal cannon bone (see image below). This system helps to prevent the shoulder from flexing and the carpus from buckling forward (flexing) when standing.
- Proximally, the biceps brachii m. attaches to the scapula via the bicipital tendon. This tendon is continuous with a central tendon running within the biceps brachii that ties distally into the connective tissue of the extensor carpi radialis m. via the lacertus fibrosus. The extensor carpi radialis m. attaches distally to the metacarpal tuberosity of the 3rd metacarpal (Mc3 aka the cannon bone).

Figure above – left forelimb, equine. Labeled structures: biceps brachii m., lacertus fibrosis, extensor carpi radialis m.
-
- Overextension of the carpus is prevented by the closely packed carpal bones and by the palmar carpal ligament adhered to the palmar aspect of the carpal bones.
-
- Overextension of the fetlock joint is prevented by the suspensory apparatus, composed of the suspensory ligament (aka interosseous tendon, see image at right [light blue structure]), proximal sesamoid bo
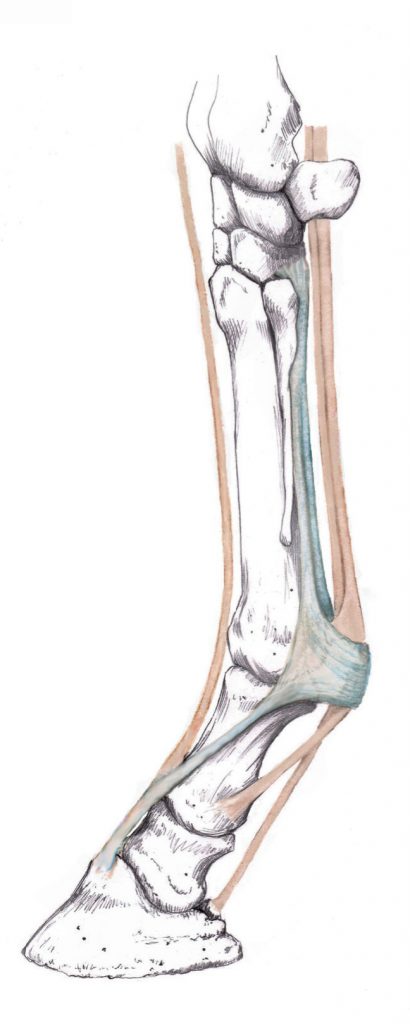 nes, and the distal sesamoidean ligaments (superficial/straight and oblique/middle, see image below Fig. 3-32).
nes, and the distal sesamoidean ligaments (superficial/straight and oblique/middle, see image below Fig. 3-32).
- The interosseous tendon originates from the palmar carpal ligament of the carpus and the adjacent portion of metacarpal 3 and divides in the distal metacarpal region into two tendons that insert on the proximal sesamoid bones (with the extensor branches coursing dorsally to join the common digital extensor m. tendon). The distal sesamoidean ligaments course from the proximal sesamoid bones to P1 and P2.
- These structures together form a sort of sling for the fetlock joint that, while allowing some stretch for normal movement, provides tension and support to the joint to prevent overextension.
- The suspensory apparatus is present in the pelvic limb as well.
- The tendons of the superficial and deep digital flexor m. also help prevent overextension of the fetlock joint by way of check ligaments. The check ligaments (proximal and distal) are connective tissue bands that tie in with the distal tendons of the superficial and deep digital flexor muscles.
-
- The proximal (radial) check ligament is associated with the superficial digital flexor m. tendon (SDFT). It attaches to the palmar surface of the distal end of the radius and then ties into the SDFT. This creates a cable that takes tension off the SDF muscle.
- The distal (carpal) check ligament is associated with the deep digital flexor m. tendon (DDFT). It attaches to the fibrous joint capsule on the palmar surface of the carpus and then ties into the DDFT. This creates a cable that takes tension off the DDF muscle.
-
- Overextension of the pastern joint is prevented via the superficial/straight sesamoidean ligament and the deep digital flexor tendon.
- Flexion of the coffin joint is prevented by the extensor branches of the suspensory ligament which join the common digital extensor m. tendon on the dorsal surface of the foot (see image below Fig. 3-36).
- Overextension of the fetlock joint is prevented by the suspensory apparatus, composed of the suspensory ligament (aka interosseous tendon, see image at right [light blue structure]), proximal sesamoid bo

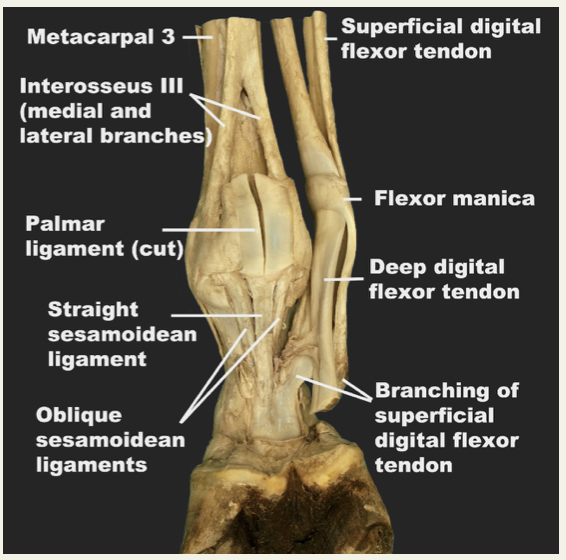
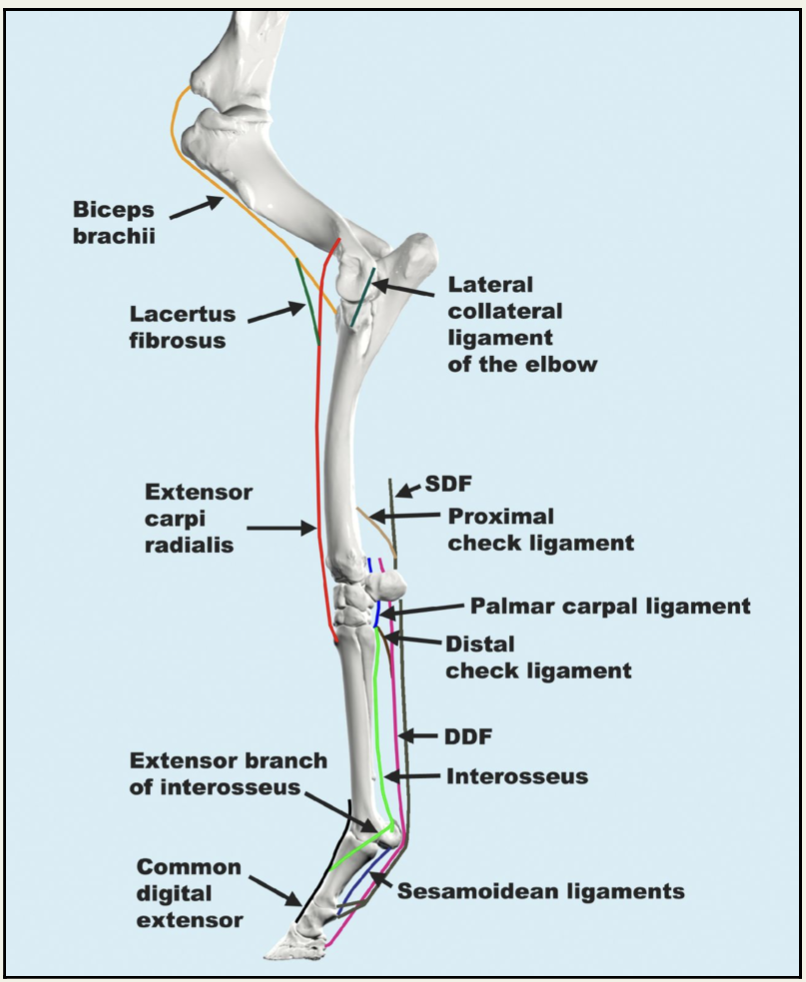
Fig. 3-36 Left forelimb, lateral view. The major components of the passive stay apparatus of the equine forelimb. This mechanism consists of a group of tendons, ligaments and fascia that prevents the bony column of the limb from collapsing under the weight of the horse. The coordinated action of these components prevents flexion of the shoulder and elbow joints, buckling forward of the carpus, and hyperextension of the fetlock and pastern. The sesamoidean ligaments (straight, oblique and cruciate) are represented by one line. SDF = superficial digital flexor; DDF = deep digital flexor (from Equine Anatomy Guide: The Forelimb; Mansour, Steiss, Wilhite)
- Clinical Notes: In high performance animals, the repetitive overextension of the fetlock joint can lead to injuries or degeneration of the suspensory apparatus (see image below, left pelvic limb).

Objective
A1.4 For each region of the forelimb, provide the name and describe the general location of the nerves innervating flexor and extensor muscle groups and identify clinical signs of nerve damage.
Nerves of the Forelimb (from the brachial plexus):
- Clinical Notes: Injury to the nerves of the brachial plexus can occur in ungulates due to the proximity of some of these nerves to bone. Injuries can also occur when ungulates accidentally get their forelimb(s) stuck or hung up and they subsequently pull back and stretch the nerves of the brachial plexus. Stretching of the nerves can also occur if the ground/floor is slippery or wet.
- Note: nerves carry motor and sensory information to and from target regions, respectively. In the most distal extent of the thoracic limbs, the nerves are mostly carrying sensory information, as there are no muscle bellies in the distal thoracic limb.
- Suprascapular n.: innervates the supraspinatus and infraspinatus mm. that stabilize the shoulder joint.
- The suprascapular n. is vulnerable to being compressed against the cranial aspect of the scapula enroute to innervate the infraspinatus and supraspinatus mm. This compression of the suprascapular n. against the cranial edge of the scapula causes nerve damage that leads to atrophy of these muscles. When the muscles atrophy, the scapular spine can be observed through the skin. (Normally, the equine scapular spine is not observable, nor even palpable, due to the bulging muscles on either side of it.) The resulting condition from the atrophy of this muscle is called “Sweeney,” (see image below, left shoulder and LAS Gait Abnormalities) and was common when lean, overworked horses pulled wagons with poorly made/poorly fitting horse collars. (The shoulder joint may appear to have increased circumduction or external rotation.) Modern day occurrences are rare, but may occur due to trauma.

- Radial n.: innervates the extensors of the carpus (extensor carpi radials, ulnaris lateralis mm.) and digits (lateral digital extensor, common digital extensor mm.). (see also LAS Nerve damage)
- The radial n. is vulnerable to being compressed against the humerus at the caudal edge of the brachialis groove. Radial nerve paralysis may be seen after recumbency when padding is not sufficient. The result is a dropped elbow and flexed fetlock with the inability to extend the elbow and digits (see image below, left forelimb).

- Median n.: innervates the flexors of the carpus (flexor carpi radialis m.) and digits (superficial digital flexor, deep digital flexor mm.). The median n. is found more medial in the forelimb as it travels distally (caudal and palmar aspects of the antebrachium and carpus). Most of the sensory information from the medial side of the foot is carried within the median n.
- Medial and lateral palmar nn. (eq) begin at the level of the carpus and continue to the distal extent of the metacarpus. The medial palmar n. runs within the carpal canal.
- Medial and lateral palmar metacarpal nn. (eq) (from the lateral palmar n.) course distally in the metacarpal region along the axial sides of metacarpals 2 and 4 to innervate the interosseous tendon and deep structures of the metacarpus and fetlock.
- Medial and lateral palmar digital nn. (eq) are continuations of the medial and lateral palmar nn., beginning at the level of the fetlock.
- The communicating branch of the medial palmar n. (eq) is found at the mid-cannon region and runs over the superficial digital flexor tendon to join the lateral palmar n.
- Medial and lateral palmar nn. (eq) begin at the level of the carpus and continue to the distal extent of the metacarpus. The medial palmar n. runs within the carpal canal.
- Ulnar n.: innervates the flexors of the carpus (flexor carpi ulnaris m.) and digits (deep digital flexor m.). The ulnar n. is found more lateral in the forelimb as it travels distally (caudal and palmar aspects of the antebrachium and carpus). Most of the sensory information from the lateral side of the foot is carried within the ulnar n.
- Musculocutaneous n.: innervates the flexors of the elbow (biceps brachii, brachialis mm.).
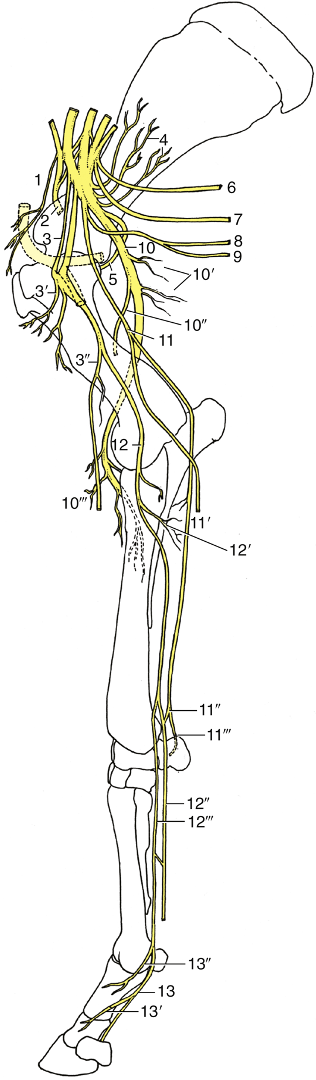
FIG. 23.43 Distribution of the nerves in the equine right forelimb, medial view. The axillary artery at the shoulder joint is stippled. 1, Cranial pectoral nerves; 2, suprascapular nerve (n.); 3, musculocutaneous n.; 3′, proximal branches; 3″, distal branches with medial cutaneous antebrachial n.; 4, subscapular n.; 5, axillary n.; 6, long thoracic n.; 7, thoracodorsal n.; 8, lateral thoracic n.; 9, caudal pectoral nerves; 10,radial n.; 10′, proximal muscular branches (triceps); 10″, lateral cutaneous antebrachial n.; 10′″, distal muscular branches; 11, ulnar n.; 11′,caudal cutaneous antebrachial n.; 11″, palmar branch; 11′″, dorsal branch; 12, median n.; 12′, muscular branches; 12″, lateral palmar n.; 12′″, medial palmar n.; 13, medial palmar digital n.; 13′ and 13″, dorsal branches.
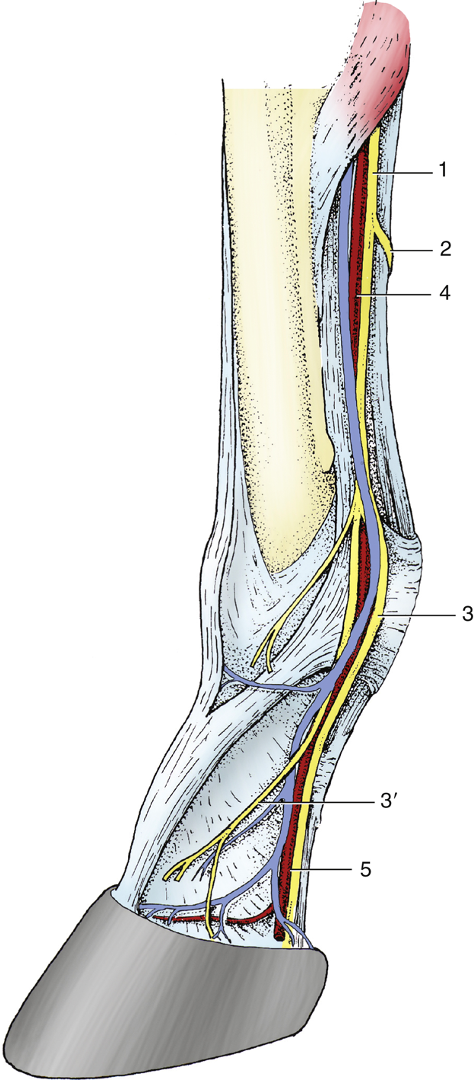
FIG. 23.45 Distribution of the equine medial palmar nerve. 1, Medial palmar nerve; 2, communicating branch; 3, medial palmar digital nerve; 3′,dorsal branch; 4, medial palmar artery and vein; 5, medial palmar digital artery and vein.
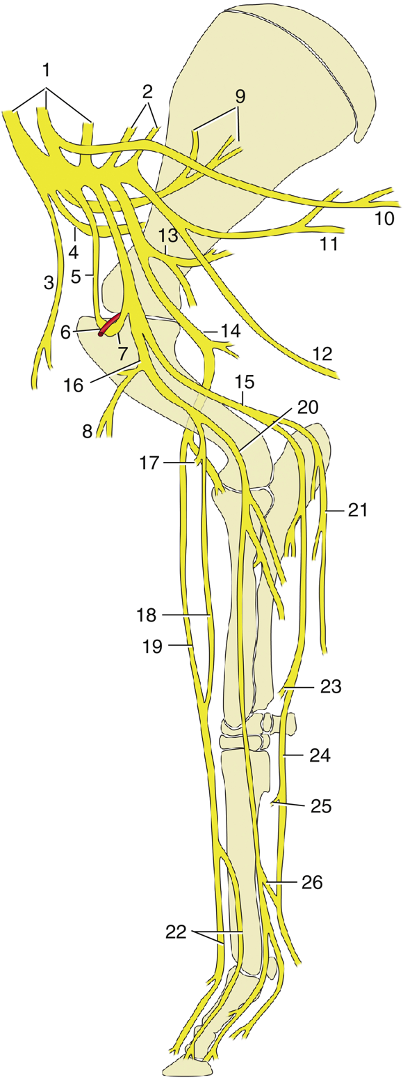
FIG. 30.15 Nerves of the bovine forelimb, medial view. 1 and 2, Roots of brachial plexus; 3, cranial pectoral nerve (n.); 4, suprascapular n.; 5, musculocutaneous n.; 6, axillary artery; 7, loop of musculocutaneous n. before joining median n.; 8, proximal branch of musculocutaneous n.; 9, subscapular n.; 10, long thoracic n.; 11, thoracodorsal n.; 12, lateral thoracic n.; 13, axillary n.; 14, radial n.; 15,ulnar n.; 16, combined musculocutaneous and median nerves; 17, distal branch of musculocutaneous n.; 18, medial cutaneous antebrachial n.; 19, superficial branch of radial n.; 20, median n.; 21, caudal cutaneous antebrachial n.; 22, dorsal common digital nerves III and II; 23, dorsal branch of ulnar n.; 24, palmar branch of ulnar n.; 25, deep branch of ulnar n. (to interosseous muscles); 26, communicating branch.
Objective
A1.5 For each region of the forelimb, identify the pathway/distribution and components of the major arterial trunk and clinically relevant veins.
Arteries
- In the limbs, arteries are in more protected locations: medially in the proximal portion of the thoracic limb (i.e., protected in the axilla), and caudally (and on the palmar aspect) in the more distal portions of the thoracic limb.
- Axillary a.: the axillary a. is a continuation of the subclavian a. The name changes to axillary after it exits the rib cage.
- Subscapular a.: this a. is found along the caudal border of the scapula and dives between the teres major and subscapularis mm.
- Cranial circumflex humeral a.: this a. runs cranially toward the shoulder and is the branch indicating the end of the axillary a.
- Brachial a.: the continuation of the axillary a. in the brachium.
- Common interosseous a.: the brachial a. gives rise to this a. distal to the elbow.
- Either the common interosseous a. (EQUINE) or cranial interosseous a. (OX) travels through the interosseous space to reach the extensors of the carpus and digits.
- Median a.: the continuation of the brachial a. in the antebrachium.
- Radial a.: the median a. gives rise to the radial a. proximal to the accessory carpal bone and carpal canal in the EQUINE (and a bit more proximal in the OX). On the palmar surface of the carpus, the radial a. runs parallel to the median a. in EQUINE.
- Medial palmar a. (eq): the median a. continues as the medial palmar a. into the metacarpal region. The medial palmar a. is the main blood supply to the digit.
- Medial and lateral palmar digital aa. (eq): the medial palmar a. divides into the medial and lateral palmar digital aa. in the distal metacarpal region, proximal to the fetlock.
- Note: in the BOVINE the naming of the distal vessels is a bit different and usually includes palmar or dorsal common digital names (there are two of each vessel type and one set of vessels for each digit). (Step #16 in Distal Thoracic Limb of the LAA Dissection eBook)
- Overview of arterial trunk in the forelimb: subclavian > axillary (changes name at cranial circumflex humeral br.) > brachial (changes name at common interosseous br.) > median (> medial palmar > medial and lateral palmar digital) aa.
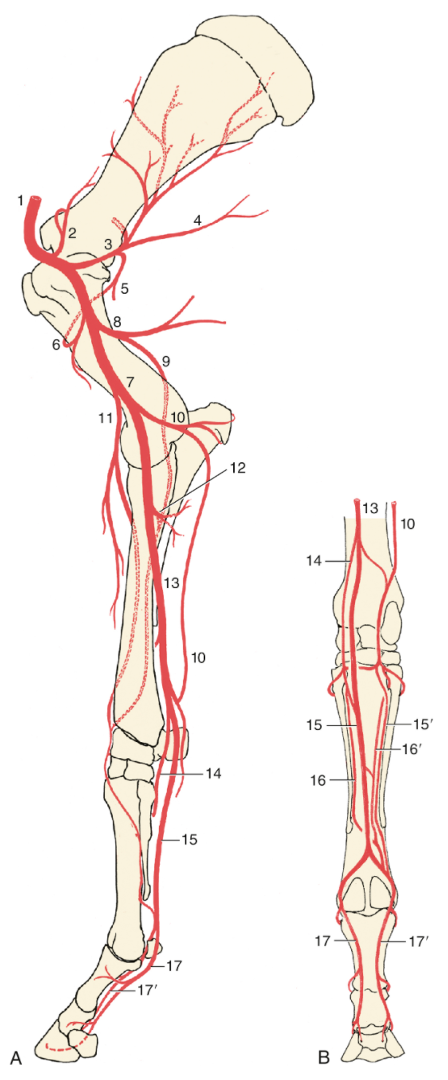
FIG. 23.39 The major arteries (aa.) of the equine right forelimb: (A) medial view; (B) palmar view. 1, Axillary artery (a.); 2, suprascapular a.; 3, subscapular a.; 4, thoracodorsal a.; 5 and 6, caudal and cranial circumflex humeral aa., respectively; 7, brachial a.; 8, deep brachial a.; 9, collateral radial a.; 10, collateral ulnar a.; 11, transverse cubital a.; 12, common interosseous a.; 13, median a.; 14, radial a.; 15 and 15′, medial and lateral palmar aa., respectively; 16 and 16′, medial and lateral palmar metacarpal aa., respectively; 17 and 17′, medial and lateral (palmar) digital aa., respectively. (TVA)

FIG. 30.13 The principal arteries on the bovine right forelimb; medial view. 1, Axillary artery (a.); 2, subscapular a.; 3, deep brachial a.; 4, brachial a.; 5, collateral ulnar a.; 6, common interosseous a.; 7, median a.; 8, radial a.; 9, palmar common digital a. III; 10, dorsal common digital a. III. (TVA)
Veins
- Superficial thoracic vein (aka spur vein) (eq): this superficial vein runs along the dorsal edge of the ascending deep pectoral m. It is just caudal to the elbow.
- Cephalic v.: the cephalic v. runs distally from the flexor surface of the carpus and drains into the external jugular v. The cephalic v. is superficial and a portion of it can be located at the border of the pectoral mm. and brachiocephalicus m. near the humerus. Sometimes the cephalic v. is used for venipuncture or insertion of catheters.
- Accessory cephalic v.: drains the dorsal aspect of the forelimb from the carpus; drains into the cephalic v. near the flexor surface of the elbow (EQUINE) or proximal to the carpus (OX).
- Median cubital v.: serves as a connection between the brachial and cephalic vv.; found on the medial surface of the elbow.
- Brachial v.: found between the biceps and triceps brachii mm. in the brachium; drains into the axillary v.
- Axillary v.: found near the wall of the rib cage in the axillary region; once it enters the thoracic cavity it becomes the subclavian v.
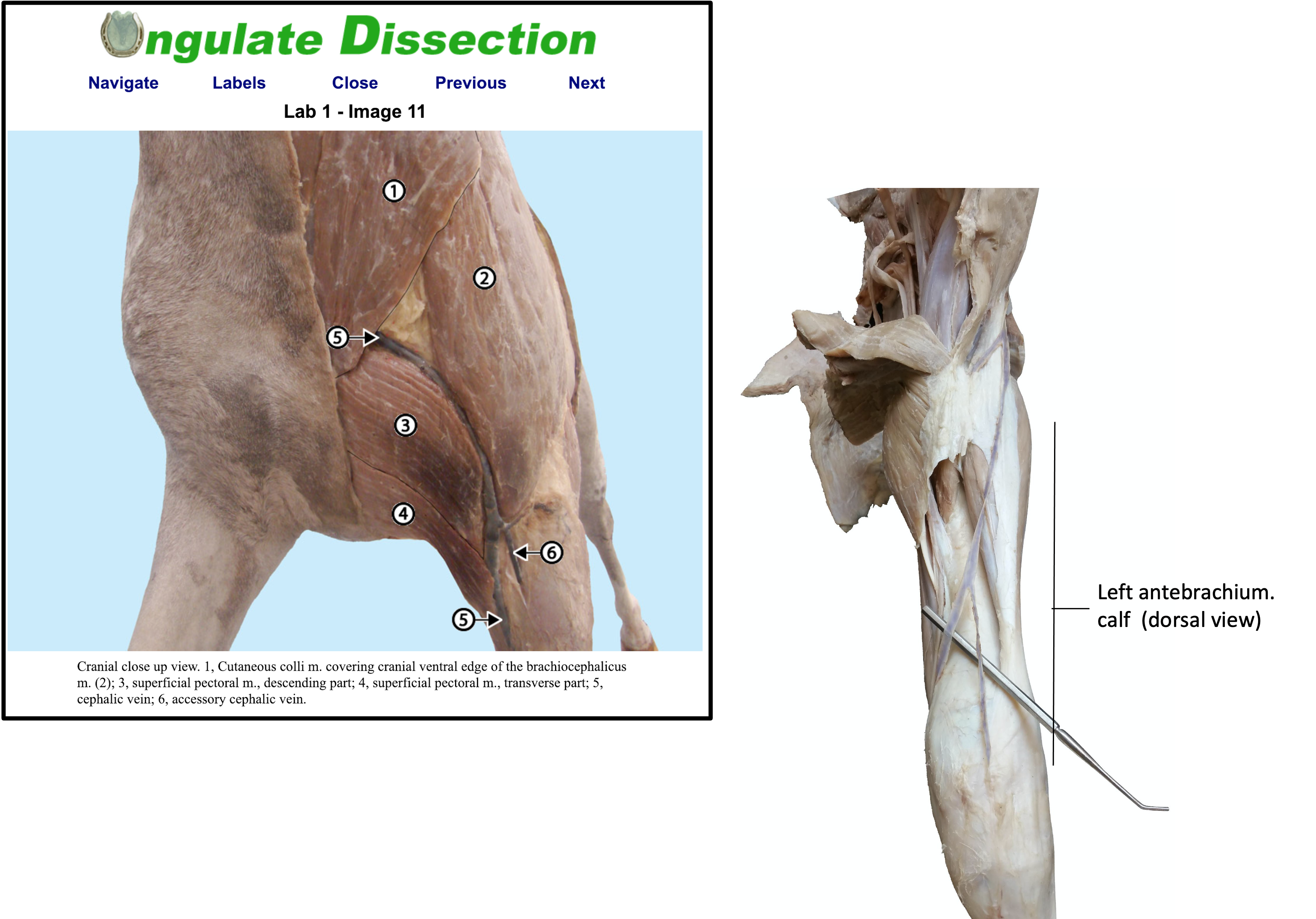
Fig (above and below): Veins in equine (left, http://vanat.cvm.umn.edu/ungDissect/Lab01/Img1-11.html) and bovine (right – image from dissection video).

Bovine Veins
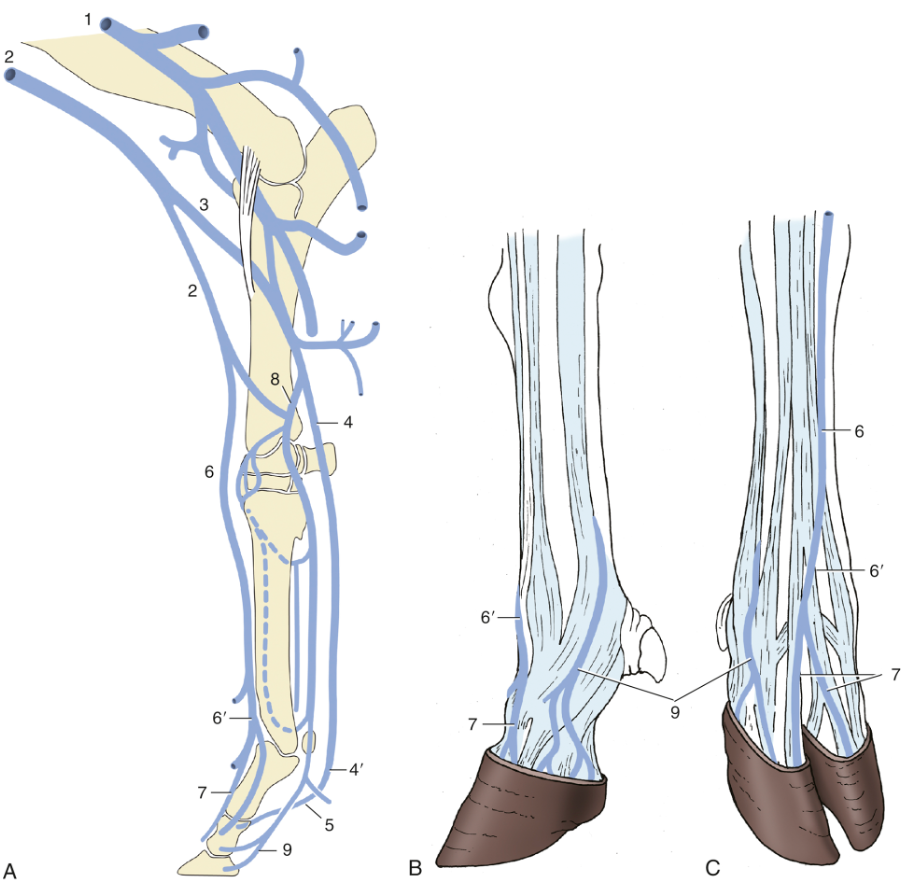
Figure 30.14 (Above) The principal veins (vv.) of the bovine forelimb. (A) Right limb, medial view. (B) Left foot, lateral view. (C) Right foot, dorsal view. 1, Brachial vein (v.); 2, cephalic v.; 3, median cubital v.; 4, median v.; 4′, palmar common digital v. III; 5, axial palmar digital vv.; 6, accessory cephalic v.; 6′, dorsal common digital v. III; 7, dorsal digital vv.; 8, radial v.; 9, abaxial palmar digital vv. (TVA)
