
Part 2: Equine Abdomen
Abby Brown
TOPOGRAPHY OF EQUINE ABDOMINAL VISCERA IN SITU
OVERVIEW — While it is important to be able to understand the viscera on the post mortem exam table, it is more important to know the normal position during life. In surgery, most identification will be by palpation rather than by sight. We will attempt to mimic this procedure by palpating the viscera through small openings in the caudal abdominal wall. In addition, the “windows” cut into the diaphragm will allow visualization of much of the viscera. There will also be isolated viscera on a table for you to manipulate and study. In the demonstration activity, you will receive further reinforcement of the anatomy through an instructor led “tour” of fresh equine viscera. The combination of these activities will allow you to learn the viscera and understand their placement within the abdominal cavity.
LOGISTICS – You will be assigned a specific time slot for the instructor led demonstration sessions. When you are not engaged in a demonstration you should go to the demonstration (prosection) specimens to palpate and view the abdominal structures and viscera. There will also be various dry museum specimens and isolated wet specimens to study and be familiar with (i.e., it is expected that there will be a lot of movement of students back and forth between demonstrations and specimens).
Table 5-1 Major structures to be palpated/seen on each side of the equine abdomen.
|
LEFT side |
RIGHT side |
|
Spleen, nephrosplenic ligament, left kidney Fundus of stomach Left dorsal colon (LDC), left ventral colon (LVC) and pelvic flexure Most of jejunum and small colon Ileum entering left side of cecum (midline) Left lobe of the liver (small) |
Base of cecum Most of liver Pylorus Descending duodenum, epiploic foramen Right dorsal colon (RDC) & right ventral colon (RVC) Cecocolic ligament |
palpation of Equine abdominal viscera in situ
The following is a summary of the two-step process you will employ to begin to understand the normal placement and structure of the equine abdominal viscera: STEP 1, Palpation and Visualization: Each person from your group should spend several minutes palpating and then yield to another group member. One person can palpate on each side simultaneously. As palpation occurs you should be discussing amongst yourselves your successes and struggles so that all will get the most out of the exercise. In so doing you will go in and out of the abdominal cavity several times. Nothing will prepare you better for abdominal surgery on a live animal than palpation opportunities such as this. STEP 2, The “Reveal”: Toward the end of lab (after all group members have done the palpation) you will incise the abdominal wall so that the contents can be dropped out of the cavity onto a table (i.e., you will be able to visualize the supporting attachment points of the viscera). This is important in understanding colic because the parts of the gut farthest from the attachment point are the most mobile, and hence, most likely to be displaced or twisted.
STEP 1, Palpation and Visualization:
- Be sure that the abdominal wall layers of the pony have been reflected as directed in Part 1 of this chapter before you prepare to palpate.
- Use a rectal sleeve (provided in lab) to cover your arm. Secure the top of the sleeve to your coveralls/lab coat/scrubs with a hemostat to help keep your arm covered as you palpate.
- When you begin, palpate without looking at the structure and then observe the structure through either the palpation access port (i.e., the hole in the abdominal wall) or the “diaphragmatic window.”
- Note that some structures will be described for observation only (i.e., they are out of reach).
- Try to keep/replace all viscera in their original position so that others can continue to palpate their normal placement after you have finished.
- You will start your palpation from one side, but before you leave that side you should also palpate the structures listed that can be palpated from either side (in the region of the pelvic inlet).
- Recall from Anatomy I that the abdominal cavity is formed by the muscles of the abdominal wall, the ribs, and the diaphragm. It is lined by peritoneum, which encloses the peritoneal cavity. The peritoneal cavity is a closed space lined by a serous membrane called peritoneum; this will include parietal and visceral layers (as well as connecting peritoneum extending between the two layers and forming mesentery).
-
As you proceed with this process, note the parietal peritoneum, which is the layer of serous membrane lining the body wall (and was incised to open the peritoneal cavity). Also note the visceral peritoneum, which is the layer surrounding/adhered to the surfaces of all of the organs within the abdominal cavity.
-
A third type of peritoneum is the connecting peritoneum that connects the parietal and visceral layers, or the visceral layers of adjacent organs. The connecting peritoneum forms peritoneal folds called ‘mesenteries’, ‘omenta’, or ‘ligaments’. We will identify various parts of connecting peritoneum as we progress through this dissection.
-
- Palpation and Visualization, LEFT SIDE: Palpate/visualize the spleen, left kidney, pelvic flexure, left dorsal colon (LDC), left ventral colon (LVC), descending (small) colon, mesenteric root, and ileum.
- On the LEFT side of the pony, (with the rectal sleeve on your right arm and referencing Figure 5-2) palpate the massive spleen and locate the wide dorsal edge, known as the base, and then the narrow apex ventrally.
- Pass your hand over the dorsal edge of the spleen and locate the nephrosplenic space dorsal to the nephrosplenic ligament which runs dorsomedially to the left kidney.
-
- Dissection Note: The nephrosplenic space is just that, a space between the base of the spleen and the left kidney. This is a potential site of ‘entrapment’ where a loop of bowel could get caught.
-
- Pass your hand over the dorsal edge of the spleen and locate the nephrosplenic space dorsal to the nephrosplenic ligament which runs dorsomedially to the left kidney.
- Find the pelvic flexure (where left ventral colon curves dorsally to become left dorsal colon) close to the pelvic inlet and note its mobility.
- Trace the left dorsal colon (LDC) and left ventral colon (LVC) forward (cranially) from the pelvic flexure.
- Note the distinct bands and sacculations on the left ventral colon.
- Find the small diameter jejunal loops, which lack bands and sacculations, and the larger diameter descending (small) colon which has a distinct antimesenteric band and sacculations.
- The descending (small) colon actually has 2 bands, mesenteric and antimesenteric; the antimesenteric band is easy to see but the mesenteric band is hidden in the attachment of the mesentery to the gut; with palpation you should be able to feel both bands.
- Trace the mesojejunum to the mesenteric root where it can twist around the axis of the root.
- Near the midline find the ileum entering the much larger cecum on its medial (left) side.
- Before withdrawing your palpation hand, identify the structures listed that can be palpated from either side, unless you have already completed this palpation from the right side.
- Observe through the left diaphragmatic window (non-palpable) that the esophageal hiatus lies between the two thick crural muscles of the diaphragm.
- Note the acute angle between the esophagus and the stomach. Also note how relatively small the stomach is compared to the overall size of the horse.
- On the LEFT side of the pony, (with the rectal sleeve on your right arm and referencing Figure 5-2) palpate the massive spleen and locate the wide dorsal edge, known as the base, and then the narrow apex ventrally.
- Palpation and Visualization, RIGHT SIDE: Palpate/visualize the cecum (base and body), right kidney, duodenum (caudal loop), liver, epiploic foramen, right ventral colon (RVC), and right dorsal colon (RDC).
- On the RIGHT side of the pony, (with the rectal sleeve on your left arm and referencing Figure 5-3) find the large base of the cecum and palpate its attachment to the dorsal body wall in the region of the right kidney.
- Note the descending duodenum that passes over the lateral side of the base of the cecum and forms a caudal loop on the caudal surface of the base of the cecum.
- Reach forward (cranially) and palpate the liver.
- Pass your hand between the liver and descending duodenum; palpate medially for a hole large enough to allow one finger to pass into it – this is the epiploic foramen, which is a possible site of small intestine entrapment.
- Dissection Note: Palpation of the epiploic foramen may not be possible in a small pony but you should be sure to observe it on the fresh viscera used for the demonstrations.
- Return to the cecum. Find the right ventral colon (RVC) leaving the base of the cecum and trace it cranially.
- By palpation, differentiate between the right dorsal and right ventral colons. Feel the distinct bands and sacculations on the ventral colon and compare it with the larger, but smooth, surface of the right dorsal colon.
- Locate the region between the terminal right dorsal colon and the cranial aspect of the base of the cecum. Note the significant connective tissue fusion of the base of the cecum to the right dorsal colon in this area, serving to indirectly anchor the end of the right dorsal colon to the dorsal body wall via the base of the cecum, which is attached to the sublumbar muscles and the right kidney.
- Reach around the caudal edge of the cecum and attempt to find the ileum entering the cecum on the medial side.
- Before withdrawing your palpation hand, identify the structures listed that can be palpated from either side, unless you have already completed this palpation from the left side.
-
Palpation and Visualization, EITHER SIDE: Palpate/visualize the pelvic brim, descending (small) colon entering the pelvic inlet, urinary bladder, uterus/ovaries (mares), and ductus deferens and vaginal ring with vessels to the testes (stallions, geldings).
- From either side, reach caudally to palpate the region of the pelvic inlet (Figure 5-4) and feel the pelvic brim (cranial edge of the pelvis/pubic region). Note how the body wall steeply declines cranial to the pelvic brim (pubic region).
- Trace the descending colon (aka small colon) into the pelvic inlet where it becomes the rectum.
- Note that the rectum is of greater diameter than the descending colon and lacks bands and sacculations.
- ALL FEMALE ponies (mares): Find the uterus and ovary (ovaries, L and R).
- Ventral to the uterine body palpate the urinary bladder.
- Note that the descending (small) colon is dorsal to the uterus as it passes into the pelvic inlet where it becomes the rectum.
- ALL MALE ponies (stallions & geldings): Note the urinary bladder and trace it back to the pelvic urethra.
- Note that equines have accessory sex glands which would be well-developed in a stallion but not in a gelding.
- Find the ductus deferens and trace it to the urethra and then back to the vaginal ring. (Recall that the vaginal ring is the reflection of the parietal peritoneum through the deep inguinal ring that surrounds the origin of the spermatic cord.)
-
- Attempt to locate the vessels of the testis on the craniolateral edge of the vaginal ring.
-
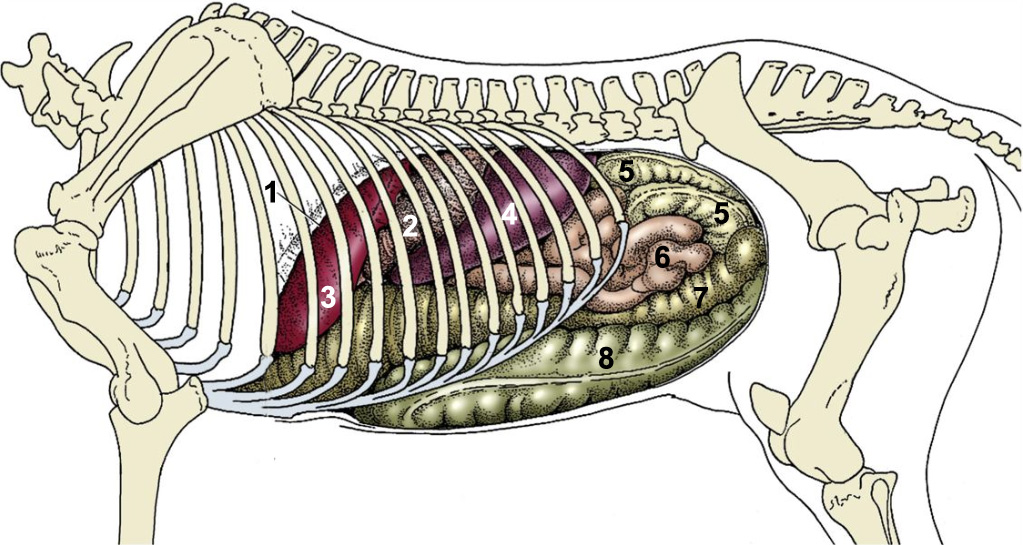
Figure 5-2. Equine, visceral projections on the left abdominal wall (including the diaphragm). 1, cut edge of diaphragm; 2, stomach; 3, liver; 4, spleen; 5, descending (small) colon; 6, jejunum; 7, left dorsal colon; 8, left ventral colon. (Modified from TVA Fig. 21-6)
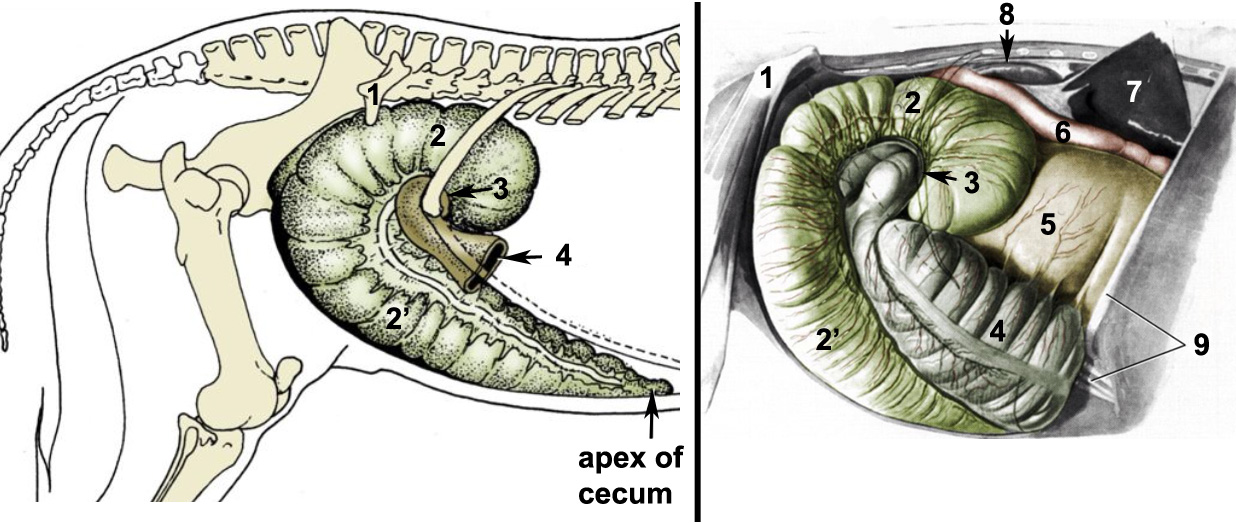
Figure 5-3. Equine, cecum and related organs lying against the right abdominal wall and flank. 1, tuber coxae; 2, base of cecum; 2’, body of cecum; 3, position of cecocolic orifice; 4, right ventral colon; 5, right dorsal colon; 6, descending duodenum; 7, right lobe of liver, elevated; 8, right kidney; 9, tenth rib and costal arch. (Modified from TVA Figs. 21-13 and 21-14)
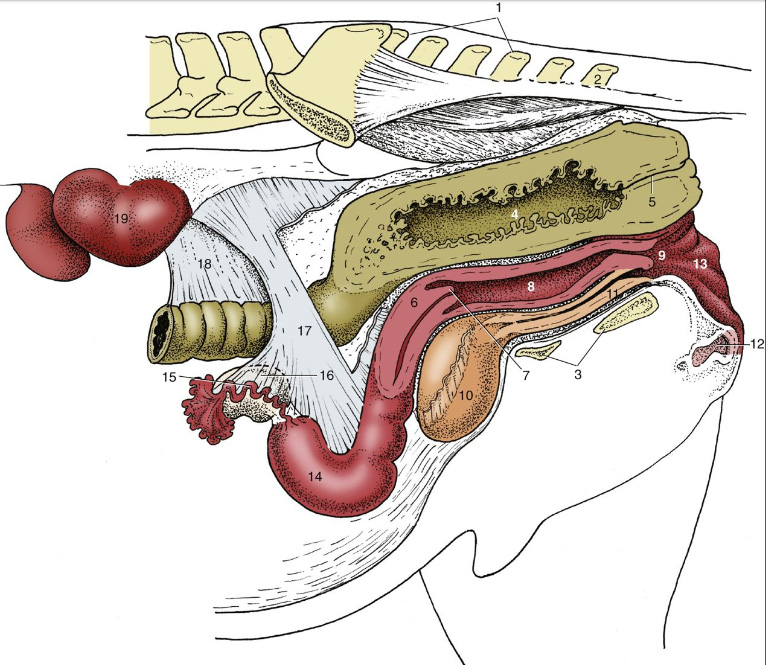
Figure 5-4. (Left) Equine, caudal abdominal and pelvic organs of the mare in situ (paramedian plane of section through pelvis). 1, sacrum; 2, Cd2; 3, floor of pelvis (cranial edge is called the pelvic brim); 4, rectum; 5, anal canal; 6, cervix; 7, vaginal part of cervix; 8, vagina; 9, vestibule; 10, bladder; 11, urethra; 12, clitoris; 13, vulva; 14, left uterine horn; 15, uterine tube; 16, ovary; 17, broad ligament (largely cut away); 18, descending mesocolon; 19, left kidney. (Modified from TVA Fig. 22-8)
STEP 2, The “Reveal”: Do this after ALL group members have palpated!
- ALL (PONY) specimens: Follow the directions outlined below to exteriorize the abdominal contents and visualize the dorsal attachment points:
- Position a table underneath the belly of the pony specimen to “catch” the viscera. (This step is especially important if you have a large pony!)
- On both sides of the pony, make vertical incisions through the abdominal wall at the level of the last rib; connect these incisions ventrally.
- ALL MALE specimens: At this point it is critical that no damage is done to the prepuce or penis as the vertical incisions are extended to the midline; be sure your connecting incision is cranial to the penis/prepuce.
- ALL FEMALE specimens: Avoid damage to the udder when connecting your incisions ventrally.
- If needed, make a ventral midline cut cranially toward the costal arch.
- Allow the viscera to drop down (onto/toward the table), but leave the dorsal visceral attachments intact. Take note of these attachments, and observe how the digestive tract is connected to the dorsal body wall.
- In general, the farther a section of bowel is from an attachment point, the greater the risk of displacement or torsion. Manipulate the small intestines to mimic rotation around the mesenteric root (aka root of the mesentery).
- Review the attachments of the base of the cecum to the dorsal body wall and the adjacent termination of the right dorsal colon.
- ALL (PONY) specimens: On the RIGHT side, open the base of the cecum with a 10cm incision and remove enough ingesta to observe the ileal orifice and the cecocolic orifice. (Figure 5-5)
-
- The ileal orifice is on the medial wall of the cecum, while the cecocolic orifice is cranial, slightly ventral, and lateral to the ileal orifice.
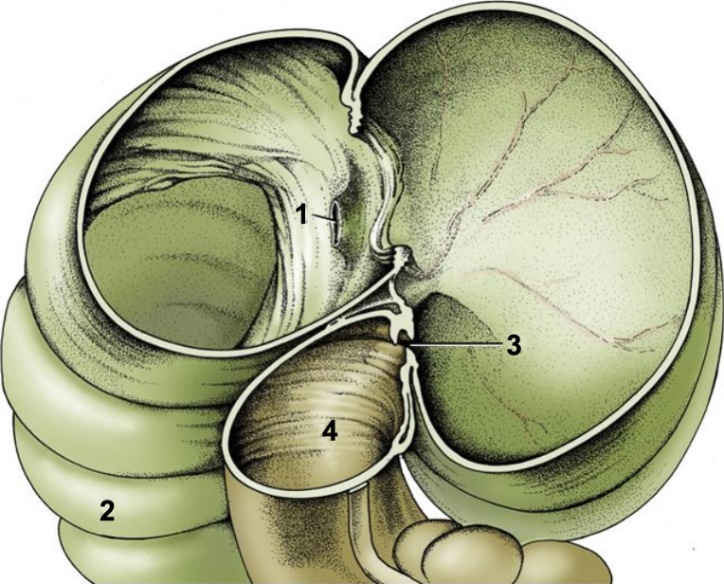
Figure 5-5. (Left) Equine. The interior of the base of the cecum, right lateral view. 1, termination of ileum at the ileal papilla (ileal orifice); 2, body of cecum; 3, cecocolic orifice; 4, right ventral colon. (Modified from TVA Fig. 21-15)
removal of pony abdominal viscera
On selected ponies (see posting in lab), remove the abdominal viscera from the specimen by following the steps outlined below. The following procedure will allow you to remove the abdominal viscera and attached major vessels en masse. Make sure that all members of your group have seen the attachment points of the viscera to the body before proceeding with this step.
- To remove the abdominal viscera en masse, sever the aorta at two points: (1) cranial to the aortic hiatus of the diaphragm and (2) cranial to the terminal bifurcation of the aorta (before the branching to the hind limbs). This will allow for the removal of the entire abdominal aorta along with the viscera.
- Sever the caudal vena cava at the same levels as the aorta.
- Cut the esophagus cranial to the esophageal hiatus of the diaphragm.
- Complete the transection of the edges of the diaphragm, cutting the costal, sternal and lumbar parts and pulling it away from the ribcage (the diaphragm will go with the viscera).
- Tie off the descending (small) colon near the pelvic inlet with two ligatures (strings) about 5 cm apart. Cut between these ligatures to protect the visceral mass from fecal contamination.
- Free the viscera from any dorsal fascial attachments and remove the abdominal viscera as a complete unit – this will include the liver, diaphragm, the abdominal aorta/caudal vena cava and both kidneys.
- As you free the viscera, the ureters will be exposed and should be cut midway between the kidneys and the neck of the urinary bladder. The urinary bladder should stay within the body, associated with the pelvis.
- Due to the weight of the viscera, removal from the abdominal cavity will involve allowing the visceral mass to descend to the table gradually.
isolated equine abdominal viscera
Use the following descriptions to help you study and identify structures of the equine abdominal viscera. Be sure to look at all available isolated specimens, which could include both embalmed and fresh equine gastrointestinal (GI) tracts as well as dried specimens.
- Spread out the viscera as shown in Figure 5-6 (below).
- In general, note that the horse has a small stomach, short small intestine, and massive colon and cecum.
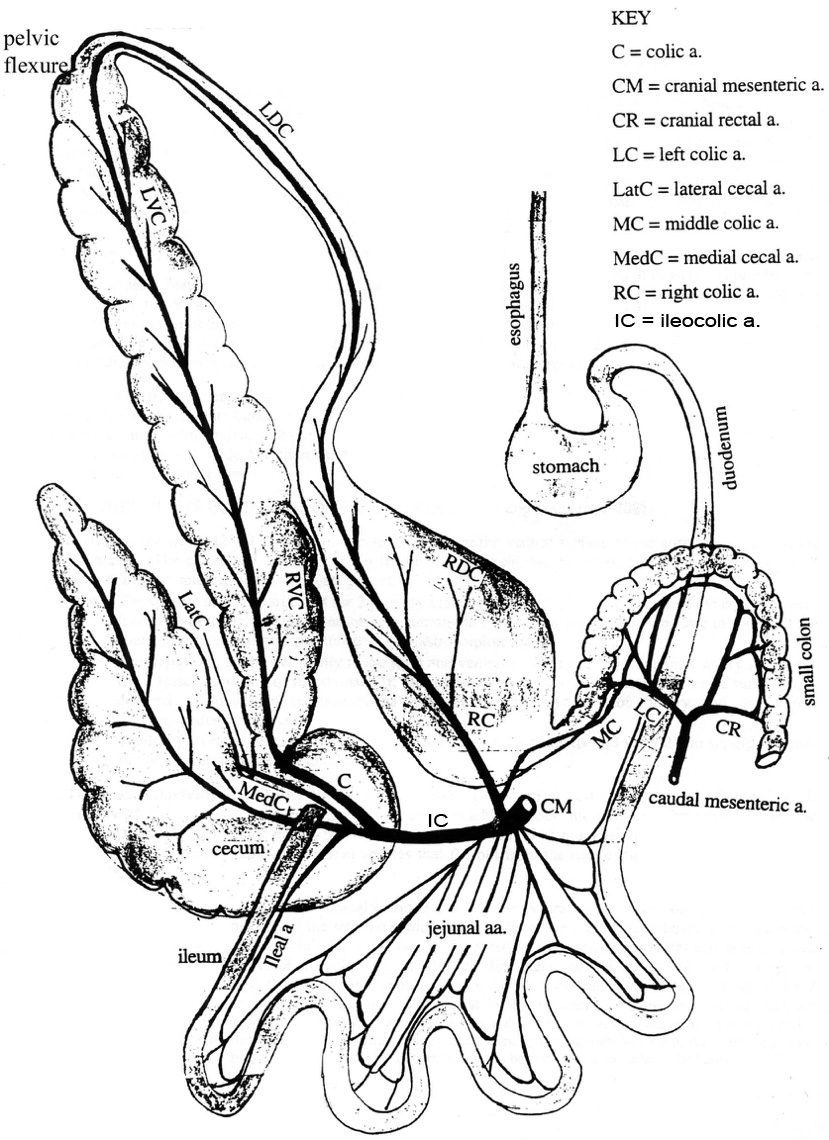
Figure 5-6. Equine gastrointestinal tract spread out for ease of study.
spleen
3. Identify the large spleen on the left side of the visceral mass and note that it has a wide base dorsally and a narrow apex ventrally.
-
- The base is attached to the left kidney by the nephrosplenic ligament (TVA 552, renosplenic).
- Clinical Note: Nephrosplenic entrapment of the left large colon in the nephrosplenic space is one of the possible causes of colic in the horse.
kidneys (Left and right)
4. In the equine, the kidneys are typically ‘heart’ shaped. Identify the left and right kidneys on the dorsal aspect of the visceral mass. The kidneys will be partially/mostly surrounded by fat. Mainly the ventral surface of the kidneys are covered by peritoneum, which is why they are considered to be retroperitoneal organs.
-
- At the hilus of each kidney, identify the ureter and look for the renal artery and vein.
- Recall from Anatomy I that the hilus is the indentation in the kidney where renal vessels and nerves, as well as the ureter, communicate with the kidney.
- Free one of the kidneys from the surrounding fat and make a longitudinal incision through the lateral border to the hilus – dividing the kidney into dorsal and ventral halves.
-
Open the kidney and identify the renal cortex and renal medulla, and note the renal pelvis.
-
Within the kidney, the outer (peripheral) layer is the renal cortex.
-
The more central, inner layer is the renal medulla.
-
Recall that the renal pelvis is the expanded part of the ureter within the kidney.
-
-
- At the hilus of each kidney, identify the ureter and look for the renal artery and vein.
liver
5. The liver lobes of the equine are less distinct than you observed in the carnivore; identify the left, right, quadrate and caudate lobes of the liver.
-
- Dissection Note: Sometimes, a round ligament of the liver can be found between the left medial lobe and the quadrate lobe. This can be a helpful landmark when identifying the liver lobes. In situ, the round ligament of the liver courses in the free border of the falciform ligament.
6. At the level of the diaphragm, open the caudal vena cava with a longitudinal incision and find the openings of the hepatic veins (draining into the caudal vena cava).
7. On the visceral side of the liver (TVA 560), attempt to find the epiploic foramen (between the right liver lobe and the duodenum) and verify that the caudal vena cava is dorsal to it and the portal vein is ventral to the foramen.
-
- Clinical Note: Entrapment of a loop of small bowel in the epiploic foramen is an occasional cause of equine colic, especially in “cribber” horses.
- Note that the caudal vena cava passes through a notch in the dorsal edge of the liver, but the portal vein terminates in the visceral surface of the liver.
8. Also on the visceral surface of the liver, note the absence of a gallbladder but find the bile duct and trace it to the duodenum.
-
- Using Figure 5-7 for reference, open the duodenum and attempt to find the orifice of the bile duct on the major duodenal papilla.
- Dissection Note: Note that you may see a minor duodenal papilla as well but it may be small/difficult to see and you need not identify it in your specimens.
- Using Figure 5-7 for reference, open the duodenum and attempt to find the orifice of the bile duct on the major duodenal papilla.
pancreas
Note that all species, including equine, have a pancreas. However, the pancreas is difficult to see/find grossly on many of the specimens, so you are not required to identify it.
Stomach
9. Identify the esophagus opening into the stomach at the cardia. Identify the fundus/fundic region (blind sac), body and pyloric regions of the stomach.
-
- Dissection Note: In situ, the cardia has a relatively fixed position close to the upper part of the 11th rib.
- Observe how close the cardia is to the pylorus, resulting in a very small lesser curvature and a correspondingly small lesser omentum.
10. Open the stomach with an incision between the greater curvature and lesser curvature, beginning with the esophagus and cardia, and extending the incision through the pylorus.
-
- Take note of the greater omentum attaching to the stomach along the greater curvature.
- Compare the thickness of the cardia with the wall thickness in the pyloric region.
- Remove the stomach contents, noting the reddish bot fly larvae if present.
- Wash out the inside of the stomach and then note that it is divided into non-glandular and glandular regions.
- The non-glandular region is stratified squamous epithelium and is found in the cardiac/fundic regions of the stomach.
- The glandular region is simple columnar epithelium and is found in the body/pyloric regions of the stomach.
- Removal of bot fly larvae results in crater-like scars in the lining of the stomach. Where are most, or all, of the larvae found (non-glandular or glandular region)? (Most are found in the non-glandular region, and along the margo plicatus, which you will identify next.)
- Note the margo plicatus, which is the boundary line between the non-glandular and glandular regions. This structure is very distinct in the equine. Be sure to view the dried specimens as well as the wet specimens to take note of this structure.
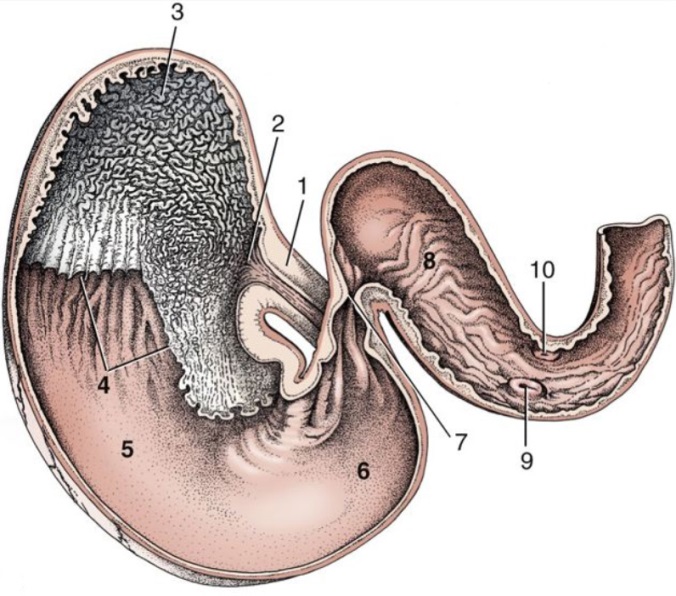 Figure 5-7. Equine, ventral caudal view of the interior of the stomach and proximal part of the duodenum. 1, esophagus; non-glandular stomach regions: 2, cardiac opening/region and 3, fundus/fundic region; 4, margo plicatus; glandular stomach regions: 5, body and 6, pyloric region; 7, pylorus; 8, cranial part of duodenum (located on the right side of abdomen); 9, major duodenal papilla; 10, minor duodenal papilla. (Modified from TVA Fig. 21-9)
Figure 5-7. Equine, ventral caudal view of the interior of the stomach and proximal part of the duodenum. 1, esophagus; non-glandular stomach regions: 2, cardiac opening/region and 3, fundus/fundic region; 4, margo plicatus; glandular stomach regions: 5, body and 6, pyloric region; 7, pylorus; 8, cranial part of duodenum (located on the right side of abdomen); 9, major duodenal papilla; 10, minor duodenal papilla. (Modified from TVA Fig. 21-9)
Small Intestine
11. After the pylorus (of the stomach), find the descending duodenum and trace it to the caudal flexure/caudal loop (of the duodenum) where it will loop around the base of the cecum and then continues as the ascending duodenum.
-
- Note the shortness of the mesoduodenum (the mesentery attached to the duodenum) that serves as a dorsal attachment to the body wall that helps the duodenum stay somewhat ‘fixed’ in its position within the body (on the right side).
- Recall that the orifice of the bile duct opens into the descending duodenum on the major duodenal papilla.
12. Trace the ascending duodenum to the jejunum, noting its long mesentery (mesojejunum).
-
- Note that the long mesojejunum allows the jejunal loops to be more mobile in the abdominal cavity, as compared to the short mesoduodenum that keeps the duodenum relatively fixed in position. The length of the meojejunum also means there can be more torsion (twisting) of the jejunal loops around the mesenteric root.
- Look for mesenteric lymph nodes located at the root of the mesentery/mesenteric root and, as you progress through the intestines, compare these with the lymph nodes associated with the large intestine which may be found at the mesenteric attachment to the large intestine.
13. Trace the jejunal loops to the ileum where it is found on the medial side of the base of the cecum and terminates in the cecum at the ileocecal orifice (aka ileal orifice).
-
- Note that the approximate length of the ileum is marked by the ileocecal fold (the fold of mesentery found between/connecting the ileum and cecum).
- The length of the ileum can vary from 10-30 inches; shortening is associated with powerful squirting of ingesta into the cecum against the gas pressure in the cecum.
- The shortened ileum may have patches of aggregated lymph nodules (not nodes) in the mucosa; these are best seen in horses less than 2 years old since, like the thymus, they regress with age.
- Palpate the ileum and jejunum and note the differences in wall thickness between the two. (The jejunum is thinner while the ileum is thicker.)
- Note that the approximate length of the ileum is marked by the ileocecal fold (the fold of mesentery found between/connecting the ileum and cecum).
14. Note that the small intestine is smooth and lacks banding compared to that found on the large intestine (which you will look at next).
large intestine
15. Identify the cecum and note that it is comma shaped and consists of the base, body and apex. (Figures 5-3 and 5-8)
-
- In the live animal, the large base of the cecum is located dorsally on the right side, and the small apex lies ventrally near the midline.
- As previously noted, the ileum empties into the cecum in the horse through the ileal/ileocecal orifice.
- Between the lesser (smaller) curvature of the cecum and the right ventral colon (RVC) find the fold of mesentery connecting the two; this is called the cecocolic fold.
- Note that the cecum empties into the colon via the cecocolic orifice.
- In the live animal, the large base of the cecum is located dorsally on the right side, and the small apex lies ventrally near the midline.
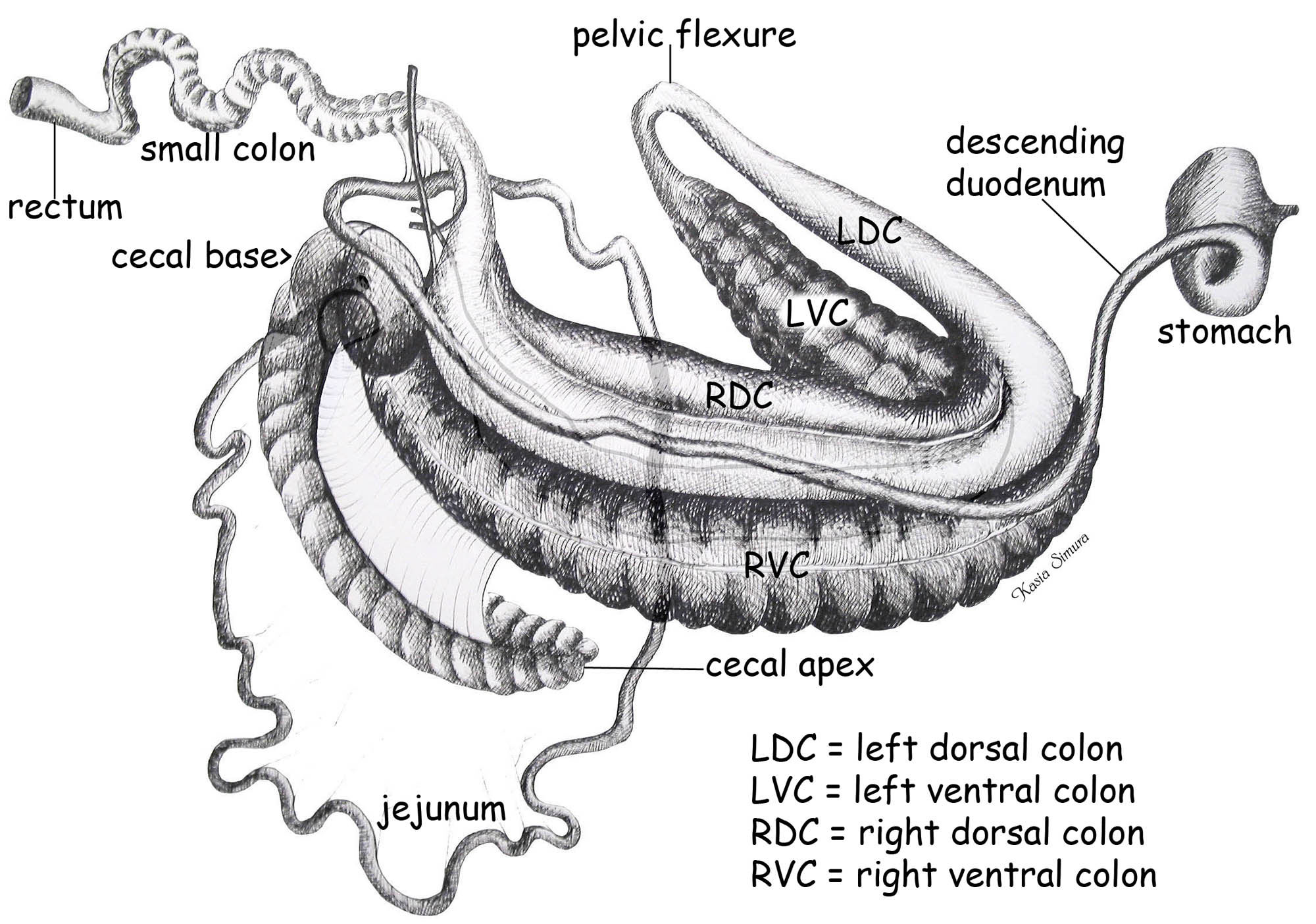
Figure 5-8. Equine intestines, viewed from the right side. (Schematic of in situ arrangement of the viscera.)
16. As noted previously, the colon of the horse is quite massive. It includes the ascending colon (with large dorsal and ventral colons), the short transverse colon, and the descending colon (aka small colon). (The descending (small) colon then terminates as the rectum.)
17. The dorsal and ventral colons represent an expansion of the ascending colon. To begin, identify the right ventral colon emerging from the base of the cecum and trace it to the left ventral colon.
-
- In situ, the right ventral colon of the large intestine takes a “U-shaped” bend (toward the left side of the body) as it passes close to the diaphragm (called the ventral diaphragmatic flexure or, referred to by some, as the ‘sternal’ flexure) to then lie on the left ventral abdominal floor as the left ventral colon.
- Note the well-developed bands and sacculations (‘haustra’ in TVA 555) on the ventral colon .
18. Tracing the left ventral colon, find the pelvic flexure (on the left side) where the ventral colon makes the bend (dorsally) to become the dorsal colon.
-
- The pelvic flexure represents a transition point from the larger diameter ventral colon to the slightly smaller diameter dorsal colon, and thus can be a likely place where impaction could occur.
- At this point you should note there is an observable sheet-like mesocolon between the ventral and dorsal colons. This mesentery between the colons is less obvious on the right side between the right dorsal and ventral colon.
19. From the pelvic flexure, trace the left dorsal colon to the right dorsal colon.
-
- In situ, the left dorsal colon of the large intestine takes a “U-shaped” bend (toward the right side of the body) as it passes close to the diaphragm (called the dorsal diaphragmatic flexure or, referred to by some, as simply the ‘diaphragmatic’ flexure) to then lie on the right side of the abdomen as the right dorsal colon.
- Note that compared to the ventral colon, the dorsal colon has indistinct/less developed bands and sacculations.
20. Review the entire section of ventral colon (right and left) and note how the right and left sides look quite similar in contrast to the dorsal colon, which is small at first (left dorsal colon) and then rapidly changes to a large size (right dorsal colon) as this section of bowel traverses from the left to the right side.
21. From the large right dorsal colon find the continuation of the large intestine, which is the small diameter transverse colon. The transverse colon then leads to the final portion of the large intestine, the descending (small) colon.
-
- Note that the transverse colon is very short and, in situ, goes from the right to the left side of the abdomen cranial to the root of the mesentery, just like in the carnivore.
- You should also note, that as the ingesta moves from the larger diameter dorsal colon into the smaller diameter transverse colon, it presents another possible impaction site in the equine.
- The descending colon (aka small colon) is very long and leads to the termination of the gastrointestinal tract at the rectum.
- Note that the descending colon has one visible antimesenteric band, one hidden mesenteric band and well-developed sacculations.
-
- Dissection Notes: The mesenteric band will be ‘hidden’ from view on the side of the descending colon that has mesentery attaching to it. However, this mesenteric band is easily palpated along the length of intestine. The very distinct antimesenteric band is visible grossly, and is seen running the length of the descending colon on the side that does not have the mesenteric attachment.
-
- Note that the descending colon has one visible antimesenteric band, one hidden mesenteric band and well-developed sacculations.
- Note that the transverse colon is very short and, in situ, goes from the right to the left side of the abdomen cranial to the root of the mesentery, just like in the carnivore.
Bands (Teniae) and SAcculations
22. Smooth muscle bands (teniae) on the large intestine are found in horses, pigs, rabbits, and primates but are most well- developed in the horse. These bands consist of discrete bundles of longitudinal smooth muscle within the outer longitudinal layer of the tunica muscularis. (Recall from microanatomy that there is also an inner circular layer to the tunica muscularis of the gut.)
-
- Where you find distinct bands (teniae) you will also see distinct sacculations of the gut wall (e.g., ventral colon) versus indistinct bands which lead to the underdevelopment or absence of these wall sacculations (e.g., dorsal colon).
- Find and count the bands on each part of the large intestine remembering that one band is always hidden by the mesenteric attachment.
- The number of smooth muscle bands is:
-
- cecum — 4 on body, 3 near apex (some bands hidden in the mesocolon)
- ventral colons — 4 distinct bands (some bands hidden in the mesocolon)
- left dorsal colon — 1 indistinct band hidden in mesocolon
- right dorsal colon — 3 wide indistinct bands (some are hidden in the mesocolon)
- small colon — 2 distinct bands (but one is hidden in the mesenteric attachment)
-
- The number of smooth muscle bands is:
Major abdominal arteries
23. The arterial branching pattern off of the abdominal aorta in the horse is very similar to the carnivore, but greatly lengthened to supply the very extensive ascending portion of the colon. The following describes some major arterial branches and the course they take within the abdomen. Refer to Figure 5-6 and be able to identify the arteries listed in bold.
24. The first major branch you should identify from the abdominal aorta is the celiac artery. This unpaired vessel arises from the ventral surface of the aorta just caudal to the aortic hiatus. Using blunt dissection, uncover the celiac a. which is only about 1 cm in length. It divides near the dorsal surface of the pancreas into 3 primary branches: splenic, hepatic and left gastric.
-
- Dissection Note: Perform this dissection on an isolated (removed) GI tract.
- The splenic a. is the largest of the 3 primary branches due to the extra-large size of the equine spleen. It courses to the left where it can be seen running in the hilus of the spleen from base to apex. Using blunt dissection, uncover and identify the splenic artery.
- Dissection Note: At the apex of the spleen, the splenic artery is continued as the gastroepiploic artery.
- The hepatic a. courses cranially to the right and then ventrally. Again, using blunt dissection, identify the hepatic artery.
- Branches of the hepatic artery supply the liver, lesser curvature of the stomach (the right gastric artery), and the greater curvature of stomach and descending duodenum (the gastroduodenal a. branching into/terminating as the right gastroepiploic artery and the cranial pancreaticoduodenal artery).
- The left gastric a. is the smallest of the 3 branches of the celiac a. and courses cranially and ventrally to supply the pancreas and lesser curvature of the stomach.
25. The second major branch to identify (arising from the abdominal aorta) is the cranial mesenteric a. This unpaired vessel arises just caudal to the celiac artery. It courses ventrally into the root of the mesentery where it quickly divides into numerous branches. Often the artery is not present as a single entity, but is represented by a clump of branches that arise directly from the aorta. Using blunt dissection, uncover the origin of the cranial mesenteric a.
-
- Dissection Note: Uncover the origin of the cranial mesenteric a. on an isolated (removed) GI tract. However, the rest of the branches from the cranial mesenteric a. (described below) can be seen/dissected on any of the specimens.
- Note that there are numerous jejunal arteries that fan out from the root of the mesentery (arising from the cranial mesenteric a.), as occurred similarly in the dog and cat; identify some of these jejunal aa. in the visceral mass.
- The ventral and dorsal colon (the portion of the gut derived from the fetal ascending colon) is supplied by the colic artery (a branch of the ileocolic a. that arises from the cranial mesenteric artery) and the right colic artery (Figure 5-6), respectively.
- These vessels anastomose with each other in the region of the pelvic flexure to form one large arterial loop. The vessels (of the arterial loop) are hidden from view in the mesocolon (the mesentery that binds ventral and dorsal colons together). You will find a mesenteric intestinal band associated with each of these colic arteries.
- Using blunt dissection, uncover and identify the colic artery supplying the ventral colon.
- Using blunt dissection, uncover and identify the right colic artery supplying the dorsal colon.
Dissection Videos for this Section of Material
Equine (Pony) Abdomen
- In situ Abdomen, Left and Right sides: https://youtu.be/oHUvRk-urG8
- Embalmed (Isolated) Abdominal Viscera: https://youtu.be/LeZd5UBVmBg?list=PLyFIwFMeNNrL2_jK2KDpW0IqNJMWxyhyF
- Fresh (Isolated) Abdominal Viscera: https://youtu.be/qhP5vQ6Kpkc?list=PLyFIwFMeNNrL2_jK2KDpW0IqNJMWxyhyF
Isolated Museum specimens
- Equine:
- Dried Stomach: https://youtu.be/Syh1hKyfV8A?list=PLyFIwFMeNNrLzhZIyY1OzY_dg1lNoOdad
- Dried Large Intestine: https://youtu.be/MJvtrBdw49Y?list=PLyFIwFMeNNrLzhZIyY1OzY_dg1lNoOdad
